NEONATOLOGY ON THE WEB
Premature and Congenitally Diseased Infants
by Julius H. Hess, M.D.
Chapter X
Diseases of the Respiratory Tract
Asphyxia Neonatorum
Asphyxia is a condition produced by any interference with
oxygenation of the blood. It may be present at birth or it may occur
subsequent to that event. Asphyxia in the new born is characterized
by an absence or feebleness of respiration which is accompanied by
cardiac action, showing that life is present. Asphyxia occurring
after birth is most frequently due to prematurity or to congenital
weakness.
During intra-uterine life the wants of the fetus are supplied from
the maternal blood stream through the placenta, oxygen being present
in sufficient quantities so that respiration is unnecessary. Normally
this state of apnea terminates at birth and respiration is
established, in all probability, as a result of the decreasing supply
of oxygen derived from the placental circulation, and of the
increasing amount of carbon dioxide which is accumulating in the
fetal blood, and upon which the stimulation of the medullary center
depends, the fetus passing from a condition of apnea to one of
dyspnea. At the same time the heart action is slowed and the
blood-pressure raised, both the result of the carbon-dioxide
stimulation. Since the respiratory center is only with difficulty
affected in the premature, it is sluggish in responding to the
increase in carbon dioxide, and if this increase is slow in
appearance respiration may not be attempted at all. Cutaneous
stimulation from extraneous influences in the outer world also plays
a part in the establishment of primary respiration.
Etiology. -- Asphyxia of the premature newborn may be due
to any one of the many causes which interfere with the oxygen supply
of the fetus either before or during labor. These causes may be
listed as follows:
- Abnormally strong and prolonged labor pains. Such lengthy and
oft-repeated uterine contractions may interferer with the exchange
of gases in the placenta or with the oxygen-laden umbilical blood
stream.
- Unequal pressure exerted by the uterus after the membranes
have ruptured, if applied to the placenta or the cord, may prevent
oxygen reaching the fetus.
- Compression or tearing of the placenta.
- Twisting or tearing of the cord or its compression while in
the uterine cavity or prolapsed.
- Premature separation of the placenta, either complete or
partial.
- Slow labor the result of weak pains or contracted pelvis.
- Premature respirations resulting from attempts at version or
from the application of forceps. In this instance the aspiration
of amniotic fluid of vaginal mucus usually forms the obstruction
to respiration.
- Maternal anemia or asphyxia from renal, cardiac, or pulmonary
affections, diseases of the blood, eclampsia or other forms of
toxemia such as are produced by morphine, chloroform, etc.
In the extra-uterine variety of asphyxia the infant
attempts respiration after birth but is unsuccessful. The reason for
this failure may be due to the presence of mucus, blood, or liquor
amnii in the respiratory passages; to the presence of anomalies of
the heart or lungs; to injuries of the skull; to the pressure from
cerebral hemorrhage; or to inherent constitutional weakness or
weakness of the respiratory muscles. In the premature infant the
respiratory center is but insufficiently developed, the respiratory
muscles are weak and the lungs are in a state bordering more or less
closely upon fetal atelectasis. All of these factors favor the
development of asphyxia, and the younger the fetal age of the infant
at the time of the birth, the more pronounced are these conditions,
though it must be remembered that not all premature infants are
debilitated (see Atelectasis).
Cerebral pressure from injuries of the skull or from intracranial
hemorrhage causes anemia of the medulla and consequently prevents
stimulation of the respiratory center with resulting lack of
respiratory activity, or with stimulation of the vagus with excessive
slowing of the pulse, which interferes with the exchange of gases
through the placenta or the lungs.
Our present belief is that the asphyxia occurring immediately
after birth is due to oxygen deficiency and to paralysis of the
respiratory center by overloading the blood with carbon dioxide. The
presence of atelectasis and pulmonary congestions and edema favors
the development of this state, which is so common in prematures and
leads to general acidosis. Ylppö demonstrated in living
premature infants alkalinity of the blood lower than that ever found
in the blood of adults. Conditions are thus favorable for excessive
acidification of the organism, not only by carbon dioxide but also by
the other acid products of metabolism. Because of the abnormal
reaction of the blood the irritability of the respiratory center is
early very reduced, leading to asphyxial attacks. In addition, it
must be borne in mind that the frequency of cerebral and spinal
hemorrhages in prematures will explain asphyxia attacks occurring in
the first two or three months of life. Finally, traumatic lesions of
the respiratory center may, in themselves, lead to disturbances in
respiration and to interference with oxygen intake.
Morbid Anatomy. -- Examination of the body of a premature
new-born infant, dead of asphyxia, shows besides the evidences of
prematurity, marked congestion of the internal organs. The right
heart, sinuses of the dura and the great vessels are filled with
blood. The brain and the organs in the thoracic and abdominal
cavities are congested and edematous. Small hemorrhages are found in
the pleura, pericardium, peritoneum, liver, kidneys, adrenals, and
retina. Occasionally effusions are seen in the serous cavities. In
the lung areas of aerated tissue are seen along with areas of
atelectasis, and the trachea and bronchi may be found filled with
mucus or amniotic fluid. Edema of the extremities and scrotum may be
present. Extravasations of blood are found in the skin and mucous
membranes as well as in the internal organs.
Symptoms. -- The strong premature infant at birth behaves
much as does the full-term healthy child; it breaths deeply, utters a
more or less vigorous cry, and the skin which at first is of a
purplish hue rapidly becomes pink. If asphyxia exists two sets of
symptoms may present themselves, depending upon the variety of
asphyxia, asphyxia livida or asphyxia pallida.
In aspyxia livida or asphyxia of the first degree the skin has a
reddish-blue or bluish tinge, the face is swollen, the eyes protrude
somewhat and the conjunctivae are injected. The extremities remain
passive though the muscles retain their tonicity or are even
hypertonic; the heart beats strongly and the apex-beat is often
apparent to the eye; the vessels of the cord are filled with blood
and pulsate; the respiratory efforts may be absent or shallow and
infrequent. These infants can be roused and made to cry, respirations
being established after suitable measures of resuscitation have been
used.
In asphyxia pallida, or asphyxia of the second degree, the
vasomotor center is overstimulated by the excess of carbon dioxide in
the blood and this overstimulation causes contraction of the
peripheral vessels with venous engorgement of the deeper vessels,
thus further overloading the heart. The face is of a waxy pallor, the
visible mucous surfaces are cyanosed, the muscle tone is lost and the
extremities hang lax. The reflex irritability is lost; there is no
attempt at respiration or at the most very feeble efforts; the
pulsations of the heart are weak and either fast or slow, and the
pulsations in the cord are absent or only weakly perceptible. The
distinguishing feature that separates this condition from asphyxia
livida is the lack of muscle tone in the pallid form, these infants
having a corpse-like appearance and only the presence of the heart
action and a few respiratory gasps show that the infant is not dead.
Further Course. -- If an asphyxiated infant is revived it
frequently remains somewhat apathetic, cries very little and does not
nurse well, requiring artificial aid in obtaining nourishment. In the
stronger infants, however, this condition tends to clear up, so that
in a few days the cry is vigorous, the movements active and the
ability to nurse is good. In the weakling, whether premature or
full-term, such improvement is much slower. The poorly developed
respiratory mechanism results in superficial and irregular breathing
and the existence of areas of atelectasis tends to delay development
of the lung. These weak infants may have breathed spontaneously at
birth though not enough to have dilated the alveoli of the lungs to a
sufficient degree and as a result repeated attacks of cyanosis occur.
These attacks of cyanosis are accompanied by a condition of apnea
which lasts a moment or longer, during which the infant ceases to
breath entirely. These attacks appear without warning and may be very
frequent in the weaker infants during the first two weeks of life,
and are evidently the result of lowered irritability of the
respiratory center. The outlook for the infant in these spells is not
good, despite the fact that treatment is undertaken, because they are
an indication of inherent weakness in the individual. In those cases
which are to recover, these attacks of cyanosis become less and less
severe and less frequent.
The after-life of these infants may be affected to some extent as
the persistence of a degree of atelectasis renders them less
resistant to infection.
Sequelae. -- Cerebral symptoms that develop later are not
at all infrequent in children asphyxiated at birth and probably
depend upon cerebral sclerosis secondary to minute intracranial
hemorrhages. Development cerebral anomalies or injuries may, however,
be primary causes of asphyxia and may later be evidenced by motor and
psychic disturbances.
Diagnosis. -- Asphyxia must be differentiated from
hemorrhage of meningeal or cerebral origin occurring during prolonged
or abnormal labor or after the application of forceps. The symptoms
of a slight hemorrhage resemble those of asphyxia, the breathing
being very superficial with frequent lapses into stupor. Convulsions
occasionally occur and the pulse may be slow or fast. Continued slow
pulse with the occurrence of coma and convulsions speak strongly for
a cerebral hemorrhage, especially after a prolonged labor or the
application of forceps. The differentiation is extremely difficult
during the first days of life in premature and weak infants and death
frequently results before the etiological factor is ascertained.
Delmas [1] recommends lumbar puncture as a
diagnostic and therapeutic measure.
Prognosis. -- The outlook for strong prematures suffering
from asphyxia livida is good, the majority recovering under proper
treatment. In the weaklings it is always grave. In asphyxia pallida
the prognosis is bad, the infant invariably succumbing if left to
itself. If the heart action improves while attempts at resuscitation
are being made it is a favorable sign. Endeavors to revive the infant
should be kept up until the heart ceases to beat. At all times undue
violence should be avoided, all attempts at resuscitation being
applied gently and at regular intervals to avoid visceral injury. If
cerebral hemorrhage is combined with asphyxia the outlook is very
poor.
The cause of death in asphyxia may be a recurrence of asphyxia
attacks, lowered irritability of the respiratory center, atelectasis
of the lung or blocking of the air passages by inspired foreign
matter or cardiac failure.
Treatment. -- The treatment of asphyxia is concerned with
clearing the respiratory passages and supplying oxygen to the
tissues. In the milder cases the finger is gently introduced into the
pharynx, or the throat stroked downward, while the child is held in
an inverted position, sufficient to clear out the obstruction to
respiration. In the cases of asphyxia livida there is usually mucus
in the trachea or bronchi, and this can frequently be removed
sufficiently to allow of respiratory activity by inverting the infant
and introducing a catheter as far as the upper opening of the larynx.
Only in the larger infants is it possible to pass the catheter into
the larynx. Suction is made with the lips and the mucus is drawn into
the catheter. Occasionally it is necessary to repeat this maneuver
several times. The dangers of a syphilitic infection are to be
remembered.
Once the passages are cleared of mucus the reflex stimulation of
respiration by external irritation is attempted. In the milder cases
the back and buttocks of the suspended child are gently slapped, cool
(90° F.) water is sprinkled over the body, or the latter is
rubbed with a warm cloth. In the severer cases the child is immersed
in hot water at a temperature of 40.5° C. (105° F.) for a
few minutes and then in a cool bath for an instant. The warm bath
relieves the vasoconstrictor spasm and the overloaded heart, the
blood being brought to the surface. Weak mustard baths, warm enemata
and careful compression of the chest are all advocated.
In the severest cases cutaneous stimulation is not sufficient and
it becomes necessary to resort to artificial respiration.
Insufflation has dangers, especially for the premature infant
whose pulmonary tissue is very delicate. If the lung is torn
emphysema follows and only a slight tear is necessary because of the
very poorly developed state of the elastic tissue in the lung of the
premature. On this account it is best to use some method by which the
amount of air to be forced into the lung may be measured. The
capacity of the lungs being about 30 cc, the use of a thin rubber
bulb of capacity smaller than this would obviate the risk of tearing
the lung tissue. The difficulty of entering the trachea of these
small premature infants must be kept in mind.
The choice of the method to be used in inducing artificial
respiration depends upon the severity of the asphyxia. There is no
use wasting time in spanking the back or making traction on the
tongue in the severer cases. In the lighter forms the simpler
measures usually suffice, but in asphyxia pallida more energetic
measures must be practised. First the air passages are cleared and
then Prochownik's method is used for thirty seconds. If this is
unsuccessful the tracheal catheter is introduced with great care and
the lungs dilated with air.
The treatment of secondary asphyxial attacks consists in the use
of warm baths, oxygen insufflations and artificial respiration. The
oxygen tank should be kept at the side of the infant's bed and either
continuous or intermittent showers of oxygen given in the attempt to
ward off cyanotic attacks (see Cyanosis).
The intracutaneous injection of oxygen with an aspirator has been
recommended in the treatment of asphyxia by Delmas.
[2] He advises injecting from 30 to 60 cc beneath
the skin, from which region it is readily absorbed with beneficial
effect. In the opinion of the author such injections, because of the
considerable trauma and shock, might result disastrously in the
treatment of premature infants.
Reanimation of asphyxiated infants by the insufflation method of
Meltzer and Auer is, according to Plauchu, quite practicable and
efficient. In this method a current of air, directed as far as the
tracheal bifurcation through a small catheter, ventilates the lungs
sufficiently to oxygenate the blood even if no respiratory movements
occur. The necessary apparatus consists of a rubber bulb, a small
mercury manometer and a No. 12 (French scale) rubber catheter. A rod
of soft copper is placed in the lumen of the catheter to give it the
proper shape for introduction and the catheter itself is marked with
transverse lines at 8, 10, and 12 cm. from the tip, indicating the
distance from the mouth to the bifurcation of the trachea in the
2000-, 3000-, and 4000-gm. child, respectively.
The method of the procedure is as follows: With the little finger
or a small gauze sponge in the hold of a forceps any mucus in the
infant's throat is removed and the child is then wrapped in a blanket
and placed with the neck slightly overextended. The index finger of
the left hand is introduced as far as the upper border of the larynx,
finding the soft opening of the glottis. The catheter is introduced
by the right hand between the tongue and the palmar surface of the
left index finger into the laryngeal opening. When it has reached the
proper distance the copper rod is removed, the insufflation apparatus
attached and air injected with the bulb, the pressure not exceeding
10 or 15 mm. of mercury.
The insufflation may be continued as long as needed. Soon the
child appears less relaxed and the heart tones become stronger and
more regular and respiratory efforts begin.
In infants weighing under 2000 gm. the larynx and trachea are
passed only with great difficulty because of their small diameter,
and the danger of secondary infection due to trauma of the tissue is
great.
The use of the pulmotor or lung motor, several modifications of
which are on the market, is not to be recommended in treating the
asphyxia of premature infants, because of the danger of rupture of
the delicate pulmonary tissue.
Cyanosis
Of all functions of the premature infant, that of respiration is
usually the least developed at birth, evidencing to a marked degree
the general lack of development of the central nervous system.
Failure on the part of the respiratory apparatus to respond in a
sufficient manner to the needs of the infant is the most frequent
cause of symptoms of the gravest nature in these weaklings and indeed
not seldom of death itself.
The underlying factors in the production of cyanosis may be
divided into inherent and extraneous. The inherent causes of
cyanosis are:
- Lack of development of the central nervous system, especially
of the respiratory center.
- Weakness of the general musculature and softness of the ribs.
- Persistence of fetal atelectasis which tends to delay
development of the lungs.
- Congenital malformations of the heart or great vessels or
myocardial asthenia.
- Malformations of the respiratory tract or of the diaphragm.
- Diseases or compression of the air passages.
- Injuries of the skull or cerebral hemorrhage.
- Obstruction to nasal breathing.
- A birth weight below 1200 gm. These infants almost invariably
suffer from attacks of cyanosis.
- Cooling of the body is given as a cause by Budin, but many
infants have a temperature of 95° F. or even 93° F.
without the occurrence of cyanosis.
- Elevation of the body temperature to more than 102° F. is
given by Zahorsky as a cause.
In the premature infant the causes among the above which are
chiefly operative in the production of the characteristic attacks of
cyanosis are the weak respiratory muscles, the softness of the ribs,
the underdevelopment of the centers of respiration and the presence
of fetal atelectasis.
Involvement of the heart is ordinarily of secondary occurrence,
the diminished amount of oxygen in the blood resulting in a slowing
and weakening of the heart's action. The atelectasis which is so
frequently present, tends to hinder the closure of the foramen ovale
and the ductus Botalli and these defects in turn predispose to
cyanosis.
The extraneous causes include:
- The aspiration of food or vomitus into the larynx or trachea.
The lack of development of the pharyngeal and laryngeal reflexes
is responsible for the food reaching the air passages and the lack
of reflex cough prevents its being ejected. Pneumonia not
infrequently follows the aspiration of such foreign particles.
- Distension of the stomach from overfeeding. This is one of the
most common causes of cyanosis and death in premature infants.
This leads to interference with the action of the diaphragm.
- Meteorism, due to
gastric and intestinal stasis.
- Attempts at drinking are often followed by cyanosis, either
the direct result of the mechanical prevention of respiration or
secondarily through the lessened oxygen content of the blood,
resulting in a lack of stimulation of the respiratory centers (von
Reuss).
- Undernourishment is strongly advanced by Budin as a causative
of cyanosis, and he has shown that with increased feeding these
attacks stop.
- An insufficient supply of water.
- The occurrence of a local or general infection.
Symptoms. -- Oftentimes, without apparent cause, attacks of
cyanosis appear with frequency during the first few weeks of the life
of the premature or weakly infant. Usually without warning the
respirations, which have previously been superficial and irregular,
become still weaker and then cease entirely for a minute or longer,
somewhat resembling the Cheyne-Stoke's type of breathing.
Accompanying the apnea is a deep cyanosis which gradually disappears
as breathing is resumed. Not infrequently, if immediate steps to
restore the respiratory activity to something like the normal are not
taken, the infant dies; in other cases breathing is spontaneously
resumed and the attack passes off, leaving the infant more or less
prostrated. Care must be taken in pronouncing it dead before
examination for heart sounds. In a few hours or days cyanosis recurs,
the attacks gradually increasing in length and severity despite
treatment, until death occurs; or they become less frequent until
they cease entirely.
Occasionally the attacks are preceded or accompanied by
convulsions. Generalized edema sometimes develops.
Diagnosis. -- From congenital cyanosis due to other causes,
or acute affections of the respiratory tract with cyanosis, these
attacks are differentiated by the history or other evidence of
premature birth, and the frequently accompanying cyanotic edema, the
respiratory weakness, absence of the normal vesicular breathing,
particularly over the bases and the tendency to a subnormal
temperature.
Prognosis. -- The prognosis of cyanosis in the premature
infant varies directly with the severity of the attacks which in turn
are more or less directly dependent upon the fetal age and the
physiological development, the ability of the infant to maintain its
body temperature, the quality of the food and the ease with which the
infant digests it.
In no other condition to which these infants are subject is the
previous training and experience of the attending nurse in the care
and handling of this class of cases, of such vast importance.
Treatment. -- A premature infant must be carefully watched
for signs of cyanosis, otherwise it may be found dead in bed. Should
an attack occur while the child is being fed, the proceeding must be
stopped and efforts made to restore respiration. The first thing to
do is to ascertain if there is any obstruction in the upper
respiratory passages. Should inspired food or vomitus be present, an
effort must be made to dislodge these particles. Inserting the little
finger into the pharynx while the child is in an inverted position
often serves to clear out the respiratory tube, and then slight
cutaneous stimulation by pinching, friction, or gentle slapping is
often enough to reinitiate breathing.
Again, exhaustion of the infant may be solely responsible for the
cyanosis. In these cases artificial respiration should be tried, the
chest being rhythmically pressed upon, or one of the other methods of
artificial respiration may be tried. Simple compression of the chest
may be tried without removal from the incubator or bed, though
removal will be found more serviceable generally.
The use of oxygen is of value in quickly reducing the degree of
asphyxia after breathing is once established, although it will not of
itself restore that function. A tank should be kept by the infant's
bed and any sign of approaching asphyxia should be the indication for
the generous shower of oxygen. The continued use of the gas when
properly applied is advocated as a valuable measure in the checking
of attacks. About 80 to 100 bubbles of oxygen gas from a partially
protected mask should escape in close proximity to the infant's
mouth.
Aromatic spirits of ammonia in one-half to two drop doses,
diluted, is of value, and nitroglycerin, one drop of a 1:1000
solution may be placed on the tongue. The use of camphor, caffein,
atropin, or other respiratory stimulants hypodermically does not
offer much practical help.
Sprinkling the baby with cool water will occasionally stimulate
respiration and as this means is always at hand it should be kept in
mind.
Infants suffering from repeated attacks of cyanosis should be
immersed in a hot bath at a temperature of 102° to 105° F.,
and subjected to gentle friction, more especially along the spinal
column. The infant may be kept in the bath for from a few seconds to
several minutes, when it should again be placed in its warmed bed,
avoiding all chilling. The efficiency of the bath may be increased by
the addition of a teaspoonful of mustard to the gallon of water. Care
should be taken to avoid aspiration of the bath water, or its
entrance into the eyes, and the danger of infection of the umbilical
cord, although not great must be kept in mind. The bath may be
repeated as indicated.
In our own experience the warm mustard bath has proven one of the
most satisfactory means of overcoming prolonged attacks. It is quite
evident that the facilities for preparing the bath must be
prearranged and great care taken to keep it at an even temperature
throughout the immersion. To facilitate handling and to prevent undue
manipulation during the cyanotic attacks the infant should be wrapped
in a blanket.
It cannot be too strongly emphasized that the manipulations
used to relieve the cyanosis should be the minimum necessary to
accomplish the result as cyanotic infants react poorly to trauma.
After an attack is over the infant should be placed in a warm
bed or bath in order to overcome the tendency to a reduction of
temperature by the previous manipulations. Afterward it is also
necessary to supervise carefully the feeding in order that two things
may be accomplished: (1) That the occurrence of further attacks of
cyanosis due to mechanical obstruction of food may be prevented; and
(2) that the nutrition of these weaklings may be immediately bettered
and thus the cyanosis indirectly controlled.
The prevention of cyanosis may be aided in several ways. The too
rapid taking of food or distension of the stomach by overfeeding must
be avoided (see Feedings). Underfeeding in cases where too frequent
feeding is undesirable can be avoided by catheter feeding at longer
intervals, although the maximum food quantities must be carefully
ascertained by starting with minimum feedings, carefully increased
according to the infant's tolerance. Catheter feeding is not well
borne by all infants and may occasionally in itself induce cyanosis.
The strength of the infant should be built up as rapidly as possible,
and the temperature of the body should be maintained by the use of
the heated bed inasmuch as a lowering of the body temperature not
only favors the development of cyanotic attacks, but makes them more
severe when they do occur. The use of oxygen may be of some value.
Insufficient supply of fluids should be avoided by the
administration of water where the fluid intake is less than one-sixth
of the body weight during the twenty-four hours.
Meteorism may be relieved by small quantities of low saline
enemata, part of which may be left in the rectum to good advantage
where the fluid intake per mouth is insufficient to meet the body
requirements.
Gastric lavage must occasionally be resorted to as a means of last
resort in overdistension of the stomach with paresis of its walls and
should be performed with the infant's head at a lower level than the
body to prevent aspiration of stomach contents, as passage of the
tube very frequently results in vomiting. This procedure is always
associated with great danger during a cyanotic attack. Occasionally
the gas can be relieved by simple passage of the catheter into the
stomach with slight pressure from without over the epigastric region.
Diseases of the Nasal Passages
The anatomy of the nasal passages of the new-born infant is such
that comparatively small degrees of swelling or accumulations of
mucus are sufficient to lead to obstruction of nasal respiration,
thereby interfering with the act of nursing. When during sleep the
tongue falls backward, thus occluding the passage between the
pillars, attacks of cyanosis and dyspnea may result.
A nasal discharge present at birth or developing within the first
two or three weeks of life should lead to a search for evidence of
congenital lues. When the syphilitic infection is sufficiently
virulent to cause premature labor the external manifestations usually
appear early.
Other sources of infection of the nasal mucosa can be found in the
passage of the child through the maternal birth canal, from the bath
water or by direct transmission from an individual suffering from a
similar infection. The organisms which may be concerned include the
various pyogenic bacteria, the pneumococcus, colon bacillus,
influenza bacillus and, less frequently, the gonococcus. The
diphtheria bacillus is frequently seen as a cause in institutional
infants.
Obstruction of the posterior nares is occasionally seen in the
new-born premature, the opening being closed by either a membranous
or a bony partition. When bilateral it favors respiratory obstruction
and may be the direct cause of attacks of asphyxia and cyanosis.
Nasal infections may threaten the infant by extension to the lower
respiratory passages, while generalized septic processes may have
their origin in a nasal infection.
Treatment. -- The prophylaxis of nasal infections
requires that if the mother is suffering from any infection of the
respiratory tract every effort should be made to prevent infection of
the offspring. Coughing or direct breathing into the infant's face
should be avoided and care taken that infectious material is not
carried from one to the other in the hand, or by means of infected
articles. The same precautions must be taken in case an attendant is
the one infected. A vaginal discharge from the mother at the time of
delivery requires that the infant's nose should be cleaned thoroughly
but carefully with a cotton pledget after birth. Lowered resistance
due to chilling of the infant is an important etiological factor and
must be avoided.
It may become necessary to remove crust formation with
instillations of normal salt or weak alkaline solutions. This must be
carefully performed to avoid forcing the infection into the
Eustachian tube and air passages, small quantities only being used.
Pledgets of cotton saturated with 1:1000 solution of adrenalin
chloride if placed within the nostril will temporarily relieve the
nasal swelling. As curative agents some of the organic silver salts
in weak solutions may be mentioned. The use of an ointment of the
yellow oxide of mercury (ung. hydrarg. ox. flav.) of 0.5 or 1 per
cent strength will be found of value. A portion the size of a small
pea should be introduced into the anterior nares and the nostril then
gently massaged in order to force the ointment as far into the nose
as possible. In cases of syphilitic or diphtheritic infectios
specific treatment must be instituted.
The breastfeeding of these infants with rhinitis offers some
difficulty because of the interference with respiration which
accompanies obstructions of the nose. Nursing at the breast is likely
to be a difficult matter under the most ideal circumstances when the
infant is as weak as many prematures are, and if added to this is an
ability to breathe while sucking and swallowing. The difficulties are
so great at times, even in infants approaching maturity, that it
becomes necessary to fed expressed milk per catheter. This method of
food administration must be instituted before the infant shows the
results of inanition.
Congenital Stridors
Congenital Laryngeal Stridor. -- In the premature infant
the presence of a stridor may go unnoticed for several days because
of the weak inspiratory effort, in contradistinction to the full-term
infant in which it is usually interpreted in the first days of life.
It must, therefore, be expected that the croaking or crowing sound
will be much more feeble than is usually heard in these cases. The
stridor usually disappears when the infant is deeply asleep, which in
the premature is the greater part of its day. Unless there is a
considerable stenosis, the infant shows no distress and cyanosis is
absent. During intense crying and in the presence of cyanotic
attacks, signs of obstruction may become evident. It is often
difficult to make an exact diagnosis in these cases because of the
dangers of direct transillumination of the larynx in these small
infants and the diagnosis is often dependent on the ability of the
clinician to exclude other causes of inspiratory dyspnea. Two cases
examined by the author at autopsy have in both instances shown
similar findings, in that there was a marked narrowing of the lumen
of the larynx with thickening of the aryepiglottic folds and
deformity of the epiglottis. Nervous disturbances due to arrested
development in the cortical centers with resulting disturbed
coordination of the act of respiration may occasionally be a
causative factor. Arrest of development affecting the center for the
recurrent nerve may also be another factor.
Treatment. -- There is usually a spontaneous functional
correction. The prophylactic care should consist in the prevention of
respiratory infections.
Stridor Thymicus. -- The frequency of true thymic
enlargement with direct tracheal pressure has undoubtedly been
exaggerated by incomplete diagnosis. The most frequent sign proving
stenosis of the upper air passages is the presence of suprasternal
retraction. In the premature the tendency of the entire chest wall to
collapse with each inspiration may be mistaken for this sign and
easily lead to an error in diagnosis. The author has seen two such
cases which were verified by palpation of a soft tumor mass in the
fossa jugularis during expiration as well as by percussion with
flatness to the right and left of the manubrium and substantiated by
roentgen-ray findings. In both cases the stridor developed shortly
after birth and disappeared spontaneously with diminution in size of
the thymus gland, both infants making an uneventful recovery. The
author has also seen a case of congenital thymus stridor in a luetic
infant which died on the sixth day. At autopsy the thymus gland
weighed 40 gm and was the seat of numerous miliary abscesses.
Prognosis. -- The prognosis varies with the cause of
enlargment. The benign forms which disappear spontaneously
undoubtedly belong to the vascular type. While the number of sudden
deaths due to causes associated either directly or indirectly with
the thymus gland are less frequent than one would be led to believe
from a review of the literature, they do occur and must be given
proper consideration. These deaths may be due to mechanical
compression of the trachea by an enlarged gland either due to true
hypertrophy or hemorrhage within the gland, or death may be caused by
hypersecretion of the gland. Syphilitic changes in the thymus with
miliary abscess formation has already been described as a cause of
death under Thymic Stridor.
Treatment. -- An expectant attitude should be adopted in
the absence of specific signs of stenosis. In the presence of
congenital lues, specific treatment should be instituted. The only
other form of treatment which offers any degree of encouragement is
that of roentgen-ray exposure in the hope of creating rapid
involution, with the development of moderate fibrosis. Friedlander
[3] describes prompt results, stating that dyspnea
is lessened even after the first treatment.
It is self-evident that exposure of premature infants to the
roentgen-ray, unless carefully guarded, may be disastrous not alone
in the too rapid atrophy of the thymus gland which is so necessary to
the growing organism, but also to the thyroid and other
parenchymatous organs as well as the danger of skin irritation.
In our wards at Michael Reese Hospital, Dr. R. A. Arens makes use
of the following equipment:
8 inch spark gap.
3 mm. aluminum filter.
10 inch S.T.D. (Skin-Target Distance)
5 M.A. (milliampères)
4 minutes exposure.
The treatment is guided entirely by the clinical course.
Frequently one or two treatments are sufficient.
Stridor from Other Causes. -- These are most commonly due
to congenital enlargement of the thyroid gland which is usually of
the vascular type and disappears spontaneously without treatment.
Congenital tracheal stenosis, deformities of the mouth, congenital
tumors of the mouth and acute inflammatory conditions of the upper
respiratory passages may be further causes.
Suffocation from External Causes
Death from suffocation due to external causes such as faulty
position (infant on face), obstruction of breathing by clothing or
overlying on the part of the parent have been responsible for the
loss of many premature and weakly infants. These have often been
described as instances of thymic death. Death from these causes is
far less common in full-term, robust new-born infants, as the latter
possess the ability to change the position of the head when
threatened with suffocation.
Affections of the Bronchi and of the Lungs
1. Congenital Anomalies
Fetal Bronchiectasis. -- Fetal bronchiectasis is a rare
condition of the new born which affects the whole or only part of one
lung. Universal bronchiectasis is the result of hydremic
degeneration of an entire bronchus, the lung structure being replaced
by cystic formations which contain a serous fluid in which are found
ciliated epithelium and nuclei.
The telangiectatic bronchiectasis is characterized by the
formation either of individual cysts or less often of multilocular
sacs, the walls of the cysts being lined with several layers of
cuboidal epithelium.
A third variety known as atelactatic bronchiectasis is due
usually to lack of development of certain portions of the lung which
later become cirrhotic from pressure from a bronchus. (Birnbaum
[4].)
Hypoplasia and Hyperplasia. -- These malformations are due
either to lack of sufficient development or to excessive development.
In hypoplasia a small airless structure is found in place of
one lung. Since the healthy lung in such cases usually grows into the
empty half of the thoracic cavity, deformity results, the thoracic
wall not developing well over the healthy lung. The same is true of
primary hypertrophy, which consists either in abnormal size or in
formation of supernumerary lobes. (Birnbaum.)
Diagnosis. -- On account of the equalizing growth of the
healthy lung the diagnosis is possible only in the presence of
deadening of the sounds over one-half of the thorax. This is much
more important in the new born than in older children, since in the
latter the above mentioned physical finding is much more significant
of an infiltration or exudation (von Reuss [5]).
Roentgen-ray studies are of assistance in localizing the lesion
although they may not determine the type of lesion.
Brochiectasis in the new born is not accompanied by any
distinctive symptoms. In the premature their existence increases the
respiratory handicap under which these infants labor, and if they are
extensive, death with symptoms of asphyxia usually occurs soon after
birth. The occurrence of inflammatory complications makes the outlook
still graver.
Atelectasis. -- Atelectasis is also spoken of as acquired
asphyxia though it may be congenital as it is a persistence of the
fetal state in all or part of the lung. In the congenital variety the
lung is not entirely expanded at birth, while in the acquired form
collapse of the previously expanded lung occurs. The congenital
variety is seen chiefly in the premature and debilitated, either due
to a developmental anomaly or insufficient strength on the part of
the respiratory muscles to inflate the lungs. The acquired form is
most frequently due to obstruction f the bronchi or alveoli by
intrathoracic exudates, diaphragmatic hernias and deformities of the
spinal column.
Atelectasis is to a degree physiological during the first few days
after birth, gradually disappearing with increasing strength. When
associated with asphyxia at birth, it is often overcome entirely by
the means used to revive the infant.
In the weak the methods used are not enough to cause complete
expansion of the lung and collapsed areas persist, the soft and
yielding thoracic wall and poorly developed respiratory muscles of
the premature both favoring the non-expansion.
The cyanosis which is so frequently seen in those suffering from
atelectasis may be directly due to the aspiration of food into the
larynx, the absence of the pharyngeal and laryngeal reflexes favoring
this. Mechanical interference with respiration during the act of
drinking may also result in cyanotic attacks; interference with the
action of the diaphragm through overdistension of the stomach (Birk
[6]) and according to Budin [7]
underfeeding, may both be responsible for cyanosis in the premature.
(See Cyanosis.)
Pulmonary atelectasis also occurs after cerebral hemorrhage, due
to injury to the respiratory center, and is characterized by small
respiratory excursions and slight exchange of gases. In the premature
the irritability of the respiratory center is low a priori,
while in those suffering from natal asphyxia it is lowered by the
asphyxia.
Pathology. -- The anterior portions of the lungs are most
frequently the portions expanded, the paravertebral parts being
atelectatic. Peiser [8] showed that in organs
hardened in situ the portion near the hilus was also
atelectatic, while the apices and borders were usually expanded, the
expanded portions often being emphysematous (Holt
[9]). When death occurred early a large portion of
the lung was usually not inflated. The left lung is usually more
atelectatic than the right. The involved parts are rich in blood and
thus form sites of predilection for inflammatory processes.
Hemorrhages and edema frequently complicate this condition, which
is made worse by the deficient heart action. These hemorrhages are
chiefly in the region of the hilus. In vessel injuries of lesser
degree there is no bleeding, only edematous extravasation.
The atelectatic lung is of brownish-red color, does not crepitate,
is very vascular and shows the lobular outline on the surface.
Usually both lungs are affected to the same degree. The heart
frequently shows the presence of a patent foramen ovale or other
congenital lesion, the liver and spleen are often congested and the
latter may be enlarged. [Fig 152]
Symptoms. -- Very frequently the subjects of atelectasis
give a history of asphyxia at birth; in others there may have been
nothing to attract attention to the lungs. Some are noticeably quiet,
cry weakly, sleep much, and their voices are feeble. The temperature
is usually below the normal; occasionally there is some edema of the
extremities or slight puffiness of the face, while the breathing is
shallow and often irregular. The gain in weight is slight or absent,
and the children remain small and delicate with poor circulation. At
any time there may develop attacks of cyanosis, which occur without
warning and which may be fatal in a few hours, often being preceded
by convulsions. These attacks may occur as late as ten or twelve
weeks after birth.
Physical Signs. -- Inspection. -- The breathing is shallow,
often irregular and at times almost ceases.
Palpation. -- This is negative unless râles are plentiful,
when fremitus may be felt. Vocal fremitus is absent.
Percussion. -- There is usually resonance over the entire chest
and only posteriorly may diminished resonance be demonstrable. The
collapsed areas are surrounded by areas which are overdistended with
air and thus resonance is not much interfered with. Small areas of
collapse give no dullness at all. If only one lung is involved a
difference can usually be made out.
Auscultation. -- The breath sounds are very feeble and the
expiratory sound in particular may be nearly inaudible. The sounds
may be rather harsher than normal, but are rarely bronchial in
character. The most marked physical sign is the presence of crepitant
râles, the so-called atelectatic crepitation, which are best
heard usually over the bases when the infant, by flagellation or
otherwise, is induced to take a deep inspiration.
Diagnosis. -- The diagnosis of atelectasis is to be made
more from the symptoms, the shallow breathing, the stupor, the
asphyxia attacks and the debilitated condition of the infant than
from the physical signs which are likely to be ambiguous and not well
defined.
If the respiratory efforts of the infant are sufficient to supply
the needed amount of oxygen the dangers from asphyxia disappear and
only the inflammatory complications which may arise in the uninflated
lung threaten its well-being. Any atelectatic area may become
inflated (bronchopneumonic) and thus areas of collapse and
bronchopneumonia may be present in the same lung. Pneumonia in an
atelectatic lung is not easy of recognition. The presence of
crepitant and subcrepitant râles, impaired resonance and the
absence of respiratory sounds, accompanied by dyspnea and ineffectual
cough, all speak of an inflammatory condition. The percussion note
may be vesiculo-tympanitic and ausculatory signs of consolidation,
such as bronchial breathing and bronchophony may be inaudible because
of the diminished respiratory excursion.
Differential Diagnosis. -- A number of conditions must be
considered in the differentiation of diagnosis, the most important of
which are the following:
General debility with quantitative and qualitative lack of
development attended with impaired respiratory cardiac and digestive
functions. This is uniformly associated with lack of development of
the thoracic wall and a tendency to collapse on the part of the
costal cartilages, and a poorly developed respiratory musculature.
Cerebral injury associated with hemorrhage is one of the most
difficult pathological conditions to differentiate, because of the
tendency toward involvement of the respiratory centers, more
especially in basilar hemorrhages. A careful inquiry should be made
for a history of opisthotonos and clonic contractions of the
extremities or facial muscles.
Hyperplasia of the thymus and occasionally the thyroid gland, with
associated stridulous respiration, retraction of the diaphragm and
local physical findings must be differentiated. When the chin is
brought down upon the chest respiration becomes more difficult and,
in turn, is made easier if the head is bent back.
Aspiration of foreign matter or food with lack of expulsitory
effort resulting in cyanosis may lead to an error in diagnosis.
Underfeeding, with secondary asphyxia.
Congenital diaphragmatic hernia.
The differential diagnosis of this condition is based on the fact
that the abdominal organs containing air enter the pleural cavity,
thus giving rise to physical signs of pneumothorax. In addition, the
following signs are presented: Respiratory movements on the affected
side are absent or less marked than normal, and there is usually
bulging of the thoracic wall on the same side; pectoral fremitus is
slight or absent and the percussion note is deep and loud and in some
cases tympanitic. Not infrequently succussion sounds can be elicited.
The normal breath sounds are absent over the affected area and the
heart is found displaced to the right. Moreover, these findings
change with a change in the position of the patient. From the
foregoing it will be seen that the findings of percussion and
auscultation are important but variable, as they depend entirely on
the amount of air or semisolid material contained in the abdominal
organs present in the pleural cavity.
Radiographic examination is of special value in differentiating
atelectasis pulmonum, hyperplasia of the thymus and diaphragmatic
hernia.
Prognosis. -- This depends upon the degree of atelectasis
which in turn usually depends upon the degree of debility of the
child. When accompanied by attacks of asphyxia and cyanosis which
appear with frequency during the first two weeks of life, the outcome
is bad, despite the institution of proper treatment, as these attacks
commonly result fatally. In favorable cases they become less frequent
and finally cease. Pneumonia in atelectatic areas often leads to a
fatal issue.
Infants who have suffered from congenital atelectasis may remain
in delicate health for a long time, although many ultimately recover
completely.
Treatment. -- The physical condition of these weaklings is
oftentimes so precarious that undue roughness in the application of
restorative measures can work infinitely more harm than they may do
good, and so it must be remembered that the less the manipulation
necessary to overcome the cyanotic attacks, the less is the danger of
injuring the infant at this critical time either by overstimulation
mechanically or by medication. The object of treatment is directed
toward the expansion of the lungs through deep breathing. This is
done by crying, and if the child does not cry strongly every day, it
should be made to do so. In the mild cases cutaneous stimulation is
sufficient, the child being very gently spanked thrice daily for
fifteen or twenty times, thus tending to expand the collapsed
portions of lung and to expel mucus from the bronchi. The mustard
bath is made by adding one tablespoon of powdered mustard to one
gallon of water at a temperature of 100° to 105° F.
Alternate immersions in warm water with a temperature of 104° F.
and cool water of 95° F. may be tried, always beginning and
ending with the warm immersions. These may be repeated at intervals
as indicated by the physical condition of the infant. The objects of
the bath are the diversion of the blood from the lungs to the
cutaneous vessels, and expansion of the collapsed areas. Expansion of
the collapsed lungs is much easier during the first few days, the
difficulty of doing this increasing proportionally with the length of
time elapsing since birth.
The infant should not be allowed to lie quietly in one position,
but its position must be changed frequently and the child picked up
several times a day. Particularly where many infants are housed with
but little individual attention atelectasis is seen most frequently.
The further treatment should be similar to that advised for attacks
of cyanosis.
As the temperature is so often subnormal, these children must be
kept warm, either by being surrounded with hot-water bottles or else
kept in some sort of heated bed. The feeding of these children is an
important problem (see chapter on Feeding). It is essential to
increase the general nutrition in order to increase the function of
the respiratory center and muscles. Aside from this, it is improbable
that increased feeding as recommended by Budin is of any direct value
as a therapeutic measure.
During attacks of asphyxia, oxygen inhalations are recommended,
and are valuable when the infant can be made to inspire, a tank being
kept in close proximity to the infant's bed. Other measures of
resuscitation mentioned under asphyxia (see Cyanosis) -- cutaneous
stimulation and artificial respiration, or even the use of forcible
means of inflating the lung with a catheter in the trachea -- may be
necessary but their danger must not be underestimated. The use of
drugs hypodermatically, such as camphor, caffeine, atropin, etc., is
not of much value. Aromatic spirits of ammonia in one-half to
three-drop doses, well-diluted, is worth trying.
Congestion and Inflammatory Changes of the Lungs.
Congestion of the Lungs. -- Congestion of the posterior
lower portions of the lung most commonly results from long-continued
rest without change of position, congenital or other anomalies of
circulation. At first there may be extravasations of serum or blood
in the alveoli and later, especially in the greater degree of
congestion, tissue infiltration.
Clinically, the condition is manifested by disturbances of
respiration, shallow breathing and asphyxial attacks. The impairment
of resonance and auscultatory findings may be confounded with those
of atelectasis or inflammations. The findings are usually bilateral
and in dependent parts; these facts aid in the differential
diagnosis. They develop post partum thereby differing from
atelectactasis and are primarily associated with fever.
Congenital Pneumonia. -- That congenital pneumonia may
exist seems to be well substantiated, although the number of cases
reported in which the infection was hematogenous and transmitted by
way of the placenta is small.
Infection of the fetus may also occur through infected amniotic
fluid before labor. However, when it is the result of the aspiration
of infectious material during the passage through the birth canal,
these cases must be classed as extra-uterine pneumonia.
Post-natal Pneumonia. -- Etiology. -- Bronchitis
during the first few days of life may be the result of aspiration of
infectious material, or it may accompany a general septic infection.
The fact that the vaginal secretion always contains microorganisms
offers every opportunity for infection, should aspiration occur
during the infant's passage through the birth canal. Infection of the
bronchi may reach the child from an infected mother or attendant, or
from a third person through the agency of feeding utensils, spoons,
or other articles. Infections in the upper air passages may spread by
direct extension to the deeper structure of the respiratory passages
and there occasion a bronchitis or bronchopneumonia.
Atelectatic areas, so common in the lungs of the premature or
weakling, and the frequency of aspiration of food or vomitus in the
debilitated favors the occurrence of pneumonic inflammation. The
richness of the atelectatic portions of the lung in blood and tissue
fluids make them a most favorable medium for the multiplication of
the invading bacteria.
The organisms found in the bronchopneumonia of early life are the
pneumococcus and staphylococcus most commonly, less frequently the
Bacillus coli, the streptococcus and the influenza bacillus.
Meyer [10] emphasizes the fact that the "grippe"
with respiratory involvement may cause a surprisingly extensive
infection.
Pathology. -- In the majority of cases both lungs are
involved, the parts most frequently affected being the lower
posterior portions. The principal lesion is an inflammation of the
walls of the bronchi, and the walls of the alveoli surrounding the
bronchi. Microscopically before section there is often no visible
evidence of consolidation, and seemingly all of the lung can be
inflated. The walls of the bronchi and alveoli are thickened and
infiltrated with round cells. The involved alveoli are filled with an
exudate which is at first composed of desquamated epithelial cells
and later of leukocytes. On section there are seen grayish-red or
yellowish-gray areas which correspond to the cut bronchi and the
surrounding peribronchitis. From the cut bronchi the fluid contents
exude, composed of epithelium, pus cells and mucus. Many of the
smaller bronchi become occluded by the excessive exudate and collapse
of the contributory alveoli follows. The collapsed portions are
depressed beneath the surface of the surrounding lung and are of a
beefy-red color.
In some cases, particularly in those instances where the
streptococcus is the causative organism, the inflammation may be of a
hemorrhagic nature. In these cases the blood vessels of the affected
areas are deeply congested, the lung tissue is studded with small
hemorrhagic patches whose size varies from that of the head of a pin
to several centimeters in diameter, the latter being true infarcts.
They are distinguished from the zone of congestion that surrounds
them by their projecting above the surrounding tissues, their dark
color and their durability. On section they are of triangular shape
with the apex more or less deeply in the lung substance. They are
seen particularly in the lower lobes. The mucous membrane of the
large and small bronchi is the seat of a catarrhal inflammation with
round-cell infiltration.
Death in the case of these prematures and weaklings is not always
the result of the virulence of the invading organism but may be
attributed rather to mechanical phenomena secondary to the
involvement of the lung. Because of the excessive amount of exudate
and intraparenchymatous hemorrhage the alveoli are filled with fluid,
the bronchial ramifications are obstructed and the gaseous exchange
limited or prevented almost entirely. Pneumonia, therefore, and
particularly hemorrhagic bronchopneumonia kills the premature by
asphyxia. In other instances death is the result of a true toxemia.
For contrast and comparison we have the recent investigations of
Ylppö [11] who found that typical
bronchopneumonic changes were very rarely observed in very young
prematures.
The following table shows the frequency of lobar pneumonia in his
series:
Frequency of Bronchopneumonia in Prematures
|
Weight
|
Death of the age of:
|
|
1 day.
|
2 days.
|
3 days.
|
4 to 15
days.
|
1 mo.
|
Older.
|
|
Under 1000 gm.
|
Number of sections.
|
14
|
9
|
2
|
6
|
2
|
1
|
|
Bronchopneumonia in these.
|
0
|
0
|
1
|
2
|
2
|
1
|
|
1000 to 1500 gm.
|
Number of sections.
|
24
|
18
|
9
|
6
|
10
|
14
|
|
Bronchopneumonia in these.
|
0
|
0
|
1
|
3
|
8
|
12
|
|
1501 to 2000 gm.
|
Number of sections.
|
10
|
1
|
8
|
3
|
3
|
16
|
|
Bronchopneumonia in these.
|
0
|
0
|
0
|
2
|
1
|
11
|
|
2001 to 2500 gm.
|
Number of sections.
|
2
|
1
|
1
|
1
|
2
|
12
|
|
Bronchopneumonia in these.
|
0
|
0
|
0
|
1
|
0
|
3
|
Ylppö's histological investigations showed that the
bronchopneumonic areas in prematures were not at all as frequent as
the bronchopneumonic areas in the full terms in the first days of
life. Hess Thaysen [12] stated that in newly born
infants dying in the first three days of life there could be
demonstrated small bronchopneumonic areas in 42 per cent of the
cases. These changes are not due to aërogenous infection but to
the aspiration of infected material from the mother during birth.
Hochheim [13] showed that the vaginal secretion and
amniotic fluid was aspirated and demonstrated the presence of foreign
bodies, as squamous epithelium, fatty bodies, meconium and lanugo
hairs in the lung alveoli.
Symptoms. -- The onset is most often insidious in the
weakly new born. At first there is noticed possibly a slight nasal
discharge and a cough of varying severity. Soon increased frequency
of respiration makes its appearance accompanied by dilatation of the
alae nasi. The cough in the more mature becomes worse and the
respiration increases to 60 or 80 per minute. Now and again slight
attacks of cyanosis occur, which in the severe cases are
correspondingly more marked. There is great restlessness in older
infants with inability to sleep, and the cyanosis becomes continuous.
Convulsions occur with more or less frequency, while the temperature
may be slightly elevated or may be subnormal even in the severest
cases. There is a marked loss of weight, the stools become dyspeptic,
and greenish with mucus and undigested particles. The prostration may
be extreme.
There is often a singular lack of symptoms and the disease may go
unrecognized. The respirations range from 40 to 60 or even 80 to 100
per minute, but are usually not labored, the pulse-rate is increased
to 140, 160, or may be uncountable; the cough may be absent entirely,
and there is often apathy and even deep stupor. The course in these
infants is usually acute, either immediate improvement or death
occurring.
The severity of these early symptoms is to be explained either on
the basis of the sudden intense congestion of the small alveoli
interfering with the bronchopulmonary apparatus almost as much as
does consolidation, or their severity may be due to the intensity of
the infection.
Physical Signs. -- The usual physical findings of a
bronchitis or bronchopneumonia are often lacking or only suggested in
the pulmonary inflammation of the premature and debilitated,
especially when the involved areas are small in size. This is due to
the fact the respiratory efforts are weak and their amplitude small.
In addition it is often the atelectatic portion of the lung which is
involved and if this is situated centrally the air may fail to gain
access to it.
On inspection there is seen more or less marked dyspnea, with
inspiratory retraction of the lower ribs; the face may be pale or
cyanosed; cough if present is frequent, short and non-productive.
Palpation may reveal nothing. Evidence of consolidation such as
increased resistance may be entirely lacking.
Percussion may give indication of consolidation if impaired
resonance or slight dullness is demonstrable, but this occurs only in
the presence of massive involvement. Occasionally the note over the
whole posterior chest may tend toward the tympanitic.
Auscultation usually offers the most reliable findings. The breath
sounds are often entirely absent over collapsed areas or the
respiratory sounds are weak and possibly higher pitched than normal.
In other instances the breathing is exaggerated, and bronchial in
character. Probably the most characteristic finding of pneumonia in
these infants is the occurrence of fine sibilant or moist
râles. These are often heard behind the lower lobes and are the
most distinctive sign of the disease. The voice sounds are, as a
rule, unchanged.
Diagnosis. -- Pneumonia may, in these infants, be easily
confused with atelectasis. If the premature infant is strong and
possesses a loud cry, congenital atelectasis may be excluded; in the
weak the latter condition is most commonly present and the physical
signs of pneumonia are absent. It must be remembered that the two
conditions may exist side by side in the same infant. It may be
necessary to make the infant cry or breath deeply by mechanical
irritation in order to bring out the various abnormal sounds. A
careful study of the history from birth may be of great assistance.
Prognosis. -- If the inflammation complicates infection in
the upper air passages, such as rhinitis or bronchitis, the outlook
is better than in primary pulmonary infections. Mixed infections with
the influenza bacillus, staphylococci and streptococci, offer a more
serious prognosis that primary pneumococcus. Involvement of a large
portion of both lungs or an extremely weakened condition of the
infant, both militate strongly against recovery. The younger the
infant the shorter the intrauterine life the higher the mortality and
when hypothermia exists death usually occurs soon. Cases which run
their course with little or no temperature are usually fatal,
probably because they occur in infants who are very feeble, of low
vitality, with limited resistance to infection.
Treatment. -- Prophylaxis. -- The prevention of
pneumonia in the premature requires that the little weaklings shall
be protected against infection from every source. The lungs are most
frequently the site of bacterial invasion, as there the organism
finds a most favorable medium for its growth. In the adult there
exist at the entrance to the respiratory tract defensive agents
capable of stopping the invading bacteria but in the premature these
defenses are absolutely rudimentary and consequently offer but slight
impediment to the entrance of pathogenic germs (Delestre
[14]).
The transmission of respiratory infections occurs by means of
infected hands or other objects or through the medium of air. No one
suffering from any infection of the nasal or respiratory passages
should handle the infant. If the mother is affected with a coryza or
bronchitis she should take care that her hands are not contaminated
with nasal or bronchial secretions and that she does not breathe, or
especially cough, in the face of the infant. A mask must be worn by
the nurse or mother if she has a respiratory infection. In
institutions where many babies are taken care of by one nurse, the
hands of the attendant should be washed before the handling of each
baby. Isolation of the premature should be practised if respiratory
affections exist among other members of the family, or in the common
wards if the infant is in an institution. Only if the attendants are
thoroughly trained in the principles of aseptic nursing is it safe to
leave the infant in close proximity to others suffering from
respiratory affections. These of all infections are hardest to
prevent. All utensils should be individual and should be sterilized
before use; feeders, spoons, glasses, nipples, bottles, stomach
tubes, etc., must all be boiled before they touch the child or its
food. The French insist on the restricted use of the incubator in the
management of premature and weak infants when the closed type is
used, and believe that their success in the handling of prematures
depends upon the fact that they remove them from the closed incubator
as soon as the body temperature reaches 37° C. and their
vitality permits. As soon as these babies can be removed from the
incubators they are kept in large, well-ventilated rooms, which are
not overheated. They should be given the benefit of open air and
sunshine as their development warrants. In favor of the open-air
treatment is the fact that most of the late deaths occur during bad
weather. The mortality drops with improved atmospheric conditions.
General Treatment. -- The treatment of pneumonia is
preëminently that of watchful expectancy, and overtreatment must
be avoided, as these feeble infants are unable to withstand
overmanipulation or stimulation. As a rule, pneumonia in robust
infants is an acute self-limited disease, but in premature infants
the course is apt to be somewhat sub-acute without the tendency to
limitation. The indications in the treatment are to support the heart
and conserve the strength. The feeding problem is difficult at any
time in the premature and during an attack of pneumonia it becomes
doubly difficult.
The hygeine of pneumonia requires that the child receive plenty of
fresh air, and to insure this in an incubator of the closed type is
difficult. The use of the open type in part overcomes this
difficulty. The position of the child should be changed frequently in
order to obviate any tendency to hypostasis. If the sick infant has
been housed in a closed incubator with questionable ventilation it
should be removed to an open, well-heated room, and placed in a
properly warmed crib or incubator bed. The prime indication is for
the promotion of elimination and sufficient administration of inert
fluid. Stimulation of the respiratory tract is best accomplished by
mild counterirritation to the chest and the use of hot applications
to the extremities. The use of drugs such as cardiac and respiratory
stimulants is not to be regarded with favor but strychnine sulphate
in 1/500 grain (0.00012 gm.) doses, or atropine sulphate in 1/2000 to
1/3000 grain (0.00006 to 0.00002 gm.) doses given hypodermically may
be of some help. The use of whisky or brandy is permissible in
quantities varying from 3 to 10 drops every two or three hours
depending upon the indications. Aromatic spirits of ammonia in 1 to
5-drop doses is one of the best stimulants at our command. Both the
whisky and the ammonia should be given well-diluted in at least 8
parts of water. In cases of emergency, of sudden heart failure or of
weakness accompanying a sudden fall in temperature, the use of
camphor-in-oil 2 to 10 minims to the dose given hypodermically will
be found to be a rapidly acting, reliable heart and respiratory
stimulant.
If the infant shows a marked rise in temperature the use of
hydrotherapy may be considered. Temperatures up to 103° F. are
well borne, and do not require interference. As a general rule the
temperature tends to remain subnormal in these weaklings and cool or
even tepid baths must be avoided and instead warm or hot mustard
baths resorted to. Even if there is an excessive amount of fever,
should it be accompanied by a cold surface, feeble pulse and shallow
respirations, cold is contraindicated. The best hydrotherapeutic
measure used for the reduction of an unduly high temperature is the
tepid pack. The use of cold baths or packs is probably never
justified in the premature or weak infant. The temperature of the
tepid bath may range from 100° to 105° F., depending upon
the condition of the child.
The treatment of attacks of collapse with cyanosis, which
are so frequent in the atelectatic prematures, should be prompt. The
infant should be immediately placed in a mustard bath (one
teaspoonful of powdered mustard mixed with one gallon of tepid water
being of sufficient strength), of about 102° to 106° F.
together with gentle massage. Respiratory and cardiac stimulants may
be needed. Oxygen should be administered continuously.
Disturbance of the nervous system, occasionally so prominent in
older and stronger children, is not marked in the premature during a
pneumonic process. When present mild hydrotherapy offers the best
results.
The use of the coal-tar products is contraindicated.
The diet is an extremely important part of the treatment of
pneumonia and will be considered under "The Feeding of the
Premature."
Frequent changes at regular intervals of the infant's position
in its bed are imperative to successful care of the pneumonias in the
premature.
Figures
|

|
Fig. 151. Specimen of thymus gland weighing 40 gm., and
resulting in thymic death.
|
|

|
Fig 152. Congenital atelectasis. Magnification of 6
diameters.
|
|

|
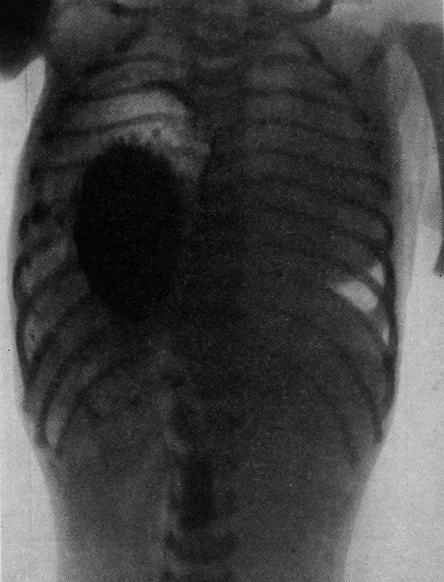
Fig. 153. Diffuse congenital atelectasis.
|
|

|
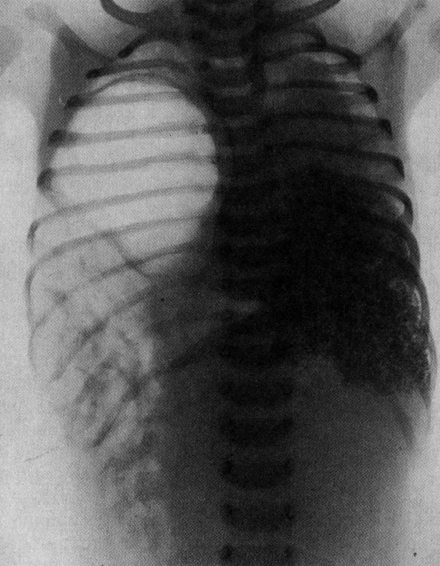
Fig. 154. Incomplete diaphragmatic hernia (case of Dr.
Irving Stein). Roentgenogram taken three and six hours after
ingestion of bismuth. Stomach and bowel in chest.
|
|

|
Fig. 155. Incomplete diaphragmatic hernia (case of Dr.
Irving Stein). Roentgenogram taken soon after death with
postmortem injection of bismuth in the bronchi. Only lower
lobe of right lung admitted the bismuth emulsion. The gas
distension of the stomach and bowels here beautifully
portrays the extent of eventration.
|
Footnotes
[1] Le Progrès médical, 1912,
40, 88-89.
[2] La médicine infantile, 1912,16,
210.
[3] Am. Jour. Dis. Child., 6, 38.
[4] Congenital Disese of the Fetus, Springer,
Berlin, 1909.
[5] Diseases of the New Born, Springer, Berlin,
1914.
[6] Leitfaden der Säuglingskrankheiten,
Marcus and Webers, Bahn, 1914.
[7] The Nursling, Caxton Pub. Co., London, 1907.
[8] Jahrb. f. Kinderh., 1908, 67, 589.
[9] Diseases of Infancy and Childhood, D. Appleton
& Co., New York, 1913.
[10] Über den Hospitalismus der
Säuglinge, Berlin, 1913.
[11] Ztschr. f. Kinderheilk., 1919, 20,
212.
[12] Jahrb. f. Kinderheilk., 1914, 79,
140.
[13] Path. Anat. Arbeiten, Berlin, 1903
(Hirschwald).
[14] Étude sur les infect. des
prématures, Thèse de Paris, 1901.
Return to the Hess Contents Page
Created 8/1/97 / Last modified 8/17/97
Copyright © 1998 Neonatology on the Web / duncan@cerf.net