Ueber Erwärmungsgeräthe für frühgeborene und schwächliche kleine Kinder (English)
Information from the obstetric clinic in Leipzig
About warming devices for premature babies and weak little children
[Ueber Erwärmungsgeräthe für frühgeborene und schwächliche kleine Kinder]
By
Credé
(With 2 woodcuts.)
Archives of Gynecology 24:128-147, 1884.

For more than 20 years, a warming tub for newborn children that I devised has been in constant use in the Leipzig maternity hospital. It is not used for full-term, strong and healthy children, because as a rule they thrive sufficiently with good, plentiful nourishment through mother’s milk and with other careful care. On the other hand, the regular supply and maintenance of heat is of the greatest importance for sickly children weakened by birth, but especially for all premature children. All such children have been protected from harmful cooling in our “warming tub” and, as we shall see later, with very favorable results.
The procedure that has been generally used up to now, to keep newborn children warm with warm towels and beds, is cumbersome and very imperfect, but other procedures, namely the use of hot-water bottles and hot-water stones, the tight, excessive tying up, the lying of the children in the bed of the Mother and the like are dangerous and have frequently caused severe burns and fatal injuries and suffocation.
It was therefore necessary to create a device which avoids such evils and dangers while being simply built and easy to monitor. I believe that I succeeded in doing this right from the start, since I have had no reason to make any changes to it over the years. In the beginning there was only one hot tub in use in the institution here, but we have had three for years, which are sometimes not enough.
The warming tub consists of a small children’s tub made entirely of good copper with a double bottom and double walls. The length measured from the outside is 75 cm above, below 65 cm, measured from the inside 60 cm above, below 55 cm; its width at the top from the outside 48 cm, at the bottom from the outside 38 cm, at the top inside 38 cm, at the bottom inside 28 cm. For the prettier look, the upper edge is curved so that the head end is slightly higher than the foot end. About 20 liters of liquid can be accommodated in the space between the double walls and the double bottom. At the highest point of the head end there is a funnel-shaped pouring opening that can be closed with a well-fitting stopper (Fig. 1 a ), at the lowest point of the foot end there is a tap that can be closed easily (Fig. 1 b) to drain the water. The filling of the interspace is carried out approximately every four hours with water heated to 40 R. = 50 C. This suffices to obtain a temperature in the interior of the tub which does not drop below 32 C., or only a little. Measurements [1] have shown that the heat between child and clothing shortly after a fresh filling is 42 C/ on average; after one hour it has dropped to 41.2 C., after two hours to 39-39.5 C., and in the last two hours it sinks somewhat faster to about 32 C. — The heat of water is just the opposite : it decreases the most in the first hour, around 10 C., and decreases by about 1.2 C. in each subsequent hour. The existing outside heat is of course of some influence. This can easily be mitigated by suitably wrapping the entire tub in materials of poor heat conduction. If, as may be desirable with children born very early, one wants to keep the warmth of the air surrounding the child at the same level as possible, this can easily be achieved by draining a part of the cooled water every hour or half an hour and pouring in warm water. Also, where the opportunity presents itself, an uninterrupted stream of warm water could be carried out, or each filling with new warm water avoided, by a small spirit, kerosene or gas flame being suitably and fire-safely placed and regulated under the bottom of the tub. Petroleum or gas flame would be installed and controlled in a practical and fire-safe manner. (I haven’t done this yet.)
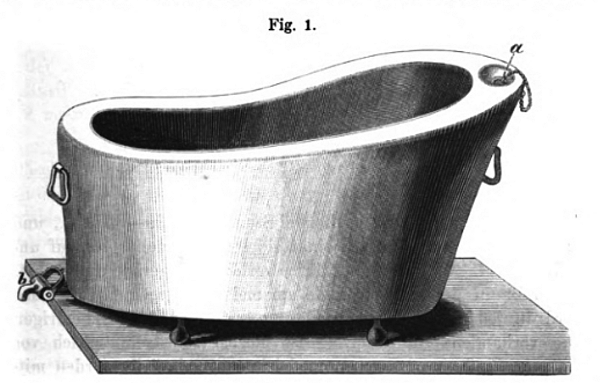
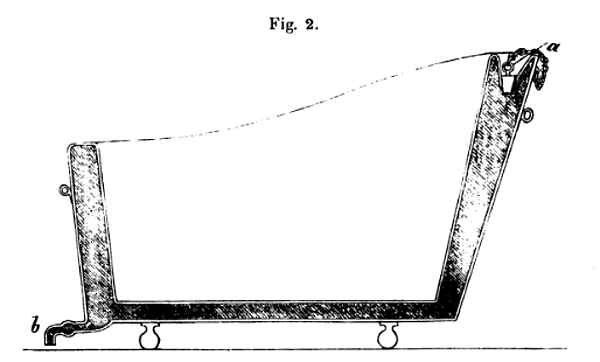
A thermometer placed between the child and the covering, and a second inserted into the water through the spout of the tub, very easily permit continuous or occasional monitoring of the degrees of heat.
When the tub is properly heated, the child, gently but generously wrapped in pure, fine cotton wool or soft flannel, is placed in it and a soft cloth or feather bed is placed on top of it, so that the inner space of the tub is completely filled. Only the child’s face remains free. The child is taken out as little as possible, only when it is to be bathed or placed on the mother’s breast. It receives any unavoidable artificial food in its warming tub, and it is usually cleaned in the same.
The warming tub stands on a bench or a low table near the stove, protected from drafts and bright light, but completely uncovered, so that fresh and cooler air can always be breathed by the child. It has two handles and can be carried around very easily because of its small size and weight, so it can be set up quickly in any room.
The children born in the institution whose weight does not reach 2500 g, or only slightly more than that, have all been bedded in it since the introduction of the warm tub. In addition, a number of somewhat larger children, who were themselves more mature, but who were ill or weakened by childbirth, also benefited from the benefits of the warming tub until they recovered. In the table below, only the prematurely born children are compiled. The table does not start until 1866 because the records in the previous years are insufficient.
Unfortunately, there are multiple gaps in the above compilation. Especially in the years 1868-1874 the medical assistants of that time neglected to register the weight of the children leaving. Furthermore, No. 171 cannot be fully utilized because the weight of the child at birth is not specified.
Before I go into more detail about the results of our observations, I would like to point out in advance that the very precise observation of the individual cases determined that the children feel very comfortable and comfortable in the warming tub: they remain evenly distributed all over their bodies, including their hands and feet warm, lying quietly, sleeping almost continuously, and generally showing normal functions. Sick, prematurely born children also make a relatively satisfactory impression in the warming tub.
It is well known that all newborn children lose weight, of course in very different degrees according to the size, maturity, health and other characteristics of the child, according to the diet, warmth, clothing and care. It is therefore scarcely feasible to compile lists of only some probative value without further consideration of the peculiarities of the individual case. However, we are reporting the results of 1200 mature, healthy children who were not cared for in the hot tub. The average weight loss during the eleven-day stay in the institution turned out to be just under 100 g. For those premature children who are listed in our table with their weight at birth and at discharge, and were all fed in the warming tub, the result was a weight loss of about 150 g. This seems to us to be an extraordinarily favorable relationship, which we have to ascribe in the main to the warming tub.
Also with regard to the number of deaths, there is a very favorable ratio for the prematurely born children cared for in the warming bath. While we found 5.5% if we calculate the mortality rate, the mortality rate for the precocious, often sick and weakened children who are cared for in the warming bath is a little over 18 percent. Unfortunately, we cannot compare these results with any number of such precocious children who have not been cared for in the warming tub. Since it was introduced, all precocious children weighing up to 2500 g have lain in the warming bath and before this time their total sum is too small for statistical evaluation.
Compilations by other observers, although not in large numbers, to which we shall return later, show that the mortality of preterm infants not cared for in warmers was 65 and 66 per cent. So this would be a very significant difference, which would speak in favor of the warming devices. But all these numbers, as I said, should only be used with caution, because they are too small in themselves and also summarize too different conditions in the individual children. It would be very worthwhile work for large maternity hospitals to compile further lists with the strictest possible separation of the peculiarities of the individual cases.
In our table of numbers, of course, the least developed prematurely born children provide the highest percentage for mortality, because of 24 who weighed 1000 to 1500 g at birth, 20 died in the institution, i.e. about 83 percent, and eight already within the first, three within the second day, two on the fifth, one each on the sixth and seventh days, two on the ninth, two on the eleventh, one on the twelfth day. The four surviving children, who weighed 1450, 1500, 1230 and 1020 g at birth, were discharged with their mothers on the 9th, 10th, 11th and 12th days.
From this it follows that children who weigh no more than 1500 g at birth can only be kept alive in very exceptional cases, even if they are given the greatest care in relation to nutrition with mother’s milk and an even supply of heat. After all, any hope of saving lives must not be given up.
Of 115 children who had weighed 1501 to 2000 g, 42 died = about 36 percent; of 476 who had weighed 2001 to 2500 g, 54 died, i.e. about 11 proc., and of 52, which had weighed 2501 to 2900 (including 17 twins), only one child died, i.e. about = 2 proc.
If we deduct the 24 children listed first from these 677 children, because such children can hardly be saved at all, then there are 97 deaths for the 653 children who weighed between 1501 and 2900 g, i.e. = about 15 percent. A very favorable result!
Unfortunately, the continued success of the warmers is greatly hampered by the inability of the maternity hospitals to house the infants longer than their mothers. However, this great nuisance also provides the best proof of the healing effect of the hot tub, because, as far as individual children could be traced further, the disadvantage of the failure of the hot tub was almost without exception immediately evident in stronger and faster coming down and very frequent deaths of the children.
If care in the warming devices can be continued punctually and without interruption for weeks or months, then numerous children who are still dying after their release from the maternity hospital will be saved alive. The warming devices are therefore recommended for foundling homes, children’s sanatoriums and above all for families.
Except for a communication intended for laypeople in the “Täglichen Rundschau, Zeitung für Nichtpolitiker 1882, November 2nd”, I have not yet published the warming tub I introduced, although it has been in use for so long. Before doing so, I wanted the largest possible number collect from experiences.
Over the years, however, my assistant doctors and students have been able to convince themselves of the usefulness of the warming tub, and I have often had the opportunity to show them to doctors from all countries who have honored the Leipzig institution with their visits. The idea and the execution were new to all, and several have since introduced my device or a similar device to their homeland. So I explained in detail to Mr. Tarnier from Paris, when he visited me in Leipzig three or four years ago, accompanied by the late Chantreuil, including my heating tub and the changes that might have to be made for private use. Tarnier [2] then had a similar device built by Odile Martin and introduced it to the Maternité de Paris. Auvard does not mention Tarnier’s visit to Leipzig.
In the main, Tarnier’s Couveuse consists of a large wooden box, with upper and lower compartments communicating with each other. The lower space contains a metal vessel for water, which is heated by a heat siphon (thermosiphon) and warms the air space surrounding this vessel; the warm air then flows into the upper room, in which the child lies in a basket. Both rooms are closed and only have small openings to allow fresh air to flow in and out. Lateral doors and a lid that can be opened are used to put in and take out the warming vessels and the child.
Anyone wishing to gain a closer knowledge of this rather artificial device should study the description and illustration in Auvard’s essay. I note, however, that a simpler and easier-to-use device is already recommended and illustrated in the same publication, and I would like to assume that the Tarnier will soon make further changes and finally to the much simpler and exactly the same function warming tub as he made in Leipzig has seen, will arrive.
Now, if we cannot take pleasure in Tarnier’s Couveuse, because of the clumsiness of the large, immovable box, because of the artificial construction, the inconvenience of service and supervision, etc., the results achieved by them are most remarkable.
As to the degree of warmth of the air in the couveuse, there does not seem to be complete agreement in Paris. At first it was raised to 34, even 35 C. in the Maternité, now 30 is taken as the average heat at Pinard, in the Hôpital Lariboisière 34 C. is considered the norm, because he noticed that only then did the limbs of the prematurely born children do not become colder than the rest of their bodies.
Budin, in the Hôpital de Charité, had a couveuse similar to the above prepared, in which the heat can be evenly maintained by a Regnard regulator. An electric bell is attached to the apparatus, which notifies the attendant that the temperature is too high.
The child in the couveuse is treated in the Maternité in the following way: Every child who is strong enough for this is fed at the breast of a wet nurse, because the mothers of the children are in rooms which are too far from the couveuse and it is too inconvenient would give to carry the Kiner so far for each suckling. Children who are too weak to suckle receive milk from donkeys, which is poured into them with a spoon or glass. All feeding bottles are banned from the Maternité. For each meal, the child is taken out of the couveuse, which must be closed again immediately, especially if, as usual, there is a second child in it. During the meal the child remains in the room air, is cleaned at the same time, if necessary, and then immediately put back into the couveuse. Meals are given every two to three hours. Children’s clothing is ordinary, diapers are changed five to six times a day, more often if erythema is present. A bath is given daily. The clothing takes place in the room air. Temporary removal from the couveuse does not appear to produce any ill effect on the children. Experiments made by Edwards on animals show that the effect of a suitable supply of heat is prolonged after the cause has ceased. So if one is often exposed to very strong cold, one bears it more easily if strong heat is supplied in the meantime. From this one could draw the conclusion for the newborns that they tolerate the cooler room heat much better after leaving a couveuse,
The children lie in swaddling gear in the couveuse. This is considered more advantageous than putting them in naked, because otherwise the children would have to be clothed every time they were taken out, but also because measurements with the thermometer have shown that while the air in the couveuse shows 30 , the heat between of the child’s skin and the diaper was 33 to 32 . So there is a warmer layer of air in the clothes than in the couveuse.
During the two years of use of the Couveuse, 151 children have lain in it. Of the 93 who were not sick and who were born prematurely, 31 died and 62 were discharged alive. Of a total of 58 prematurely born children, who were suffering from very different diseases at the same time, 15 died and 43 were discharged alive. The results for each disease are also given. But the numbers are far too small to be of any statistical value. The remark that the children who survived were mostly in good condition when they were released must be considered sufficient for the time being.
Altogether there were 151 cases with 105 children alive and 46 children dead.
The investigations made in the Maternité into the influence of the couveuse on the breathing, the pulse, and the body heat of the newborn have probably not yet reached a satisfactory conclusion, but they do contain results that are worth estimating.
Since the introduction of the couveuse in the Maternité, all but a few children weighing less than 2000 g have been cared for in the couveuse.
For comparison, the successes in children who were under the same circumstances and who were in the usual atmosphere are compiled, namely 1) in the Maternité de Paris from April 1, 1879 to July 31, 1881 (i.e. until the introduction of the couveuse), and 2) in the Maternité de Cochin during 1882. It turns out that using the couveuse the mortality rate was 38%, amounted to 66% in the Maternité de Paris, and 65% in the Maternité de Cochin without application of the same.
The successes achieved in Leipzig cannot be compared with Tarnier’s, because we nursed all children up to 2500 g and some with even greater weights in the warming tub, while Tarnier drew the limit at 2000 g.
But I don’t think I’m making a false conclusion if I assume that the percentage of 18 deaths that we achieved in Leipzig with the heating tub, despite the fact that children weighing up to 2500 g and more were cared for in it, will be just as favorable as the one won in the Maternité de Paris with the couveuse of 38 proc. in children up to 2000 g weight. In any case, both results are very satisfactory and call for the most extensive use of suitable warming devices.
If we compare the construction of the Leipzig warming tub with the Paris Couveuse, I consider the Leipzig tub to be more suitable for more general use in that it is much simpler, easy to carry from one room to another like any tub, i.e. always in the same room. where the mother is, also because the child hardly needs to be removed from the tub and because fresh, not too hot air can flow to him for breathing, better than in the couveuse.
One could object that both the Leipzig tub and the Paris couveuse will only be used in maternity wards because they are too expensive. The Leipzig tub can, however, be very easily made from cheaper material, if not to the same degree of perfection, and if necessary it can also be put together in such a way that a smaller tub or a tub-like household utensil can be fitted into an ordinary, not too small wooden or metal children’s bathtub Zinc, copper, glass, or china, but capacious enough to accommodate the child comfortably in its cloaks and covers, so placed and fastened or weighed down that it cannot swim when the warm water has been poured into the larger vessel . It is recommended to place under the smaller vessel in which the child is to lay a few flat stones, iron rods, or the like, in order to form a layer of warm water under the vessel as well. Changing the water frequently is easy to do. The use of the hot-tub at its best may be made possible even for poor people, if plumbers or bandagists keep the equipment in stock for loan to families.
The first Tarnier couveuse, on the other hand, has proven itself for maternity, but is much too expensive for family needs and, in particular, too clumsy and cumbersome. In our opinion, the second simpler couveuse, intended by Tarnier more for family use, does not yet fulfill its purpose and will hardly gain the desired acceptance in families.
More recently, Winckel had a device built [3] to keep premature, weak and sick children in warm water baths continuously or with minor interruptions for days. I refer to the original writing and the illustration, since the device can hardly be made understandable without the latter.
The six experiments reported by Winckel had very favorable results, especially with regard to the slight decrease in the children’s weight. The very artificially constructed apparatus requires almost uninterrupted supervision day and night, and is therefore hardly suitable for more general use. In addition, the pollution of the water, the cumbersome storage and removal, and the forced position of the child seem to us to be serious inconveniences. In any case, a lot of experience with the device still has to be made before a decision can be made about its usefulness. In cases where more emphasis is placed on the water than on the heat, it is more convenient, and probably with equal success, in my opinion, besides the use of the warming tub,
Finally I mention a communication from Clementovsky [4], chief physician of the Imperial Foundling Hospital in Moscow. After emphasizing heat among the external means for strengthening the blood circulation in prematurely born children, especially in those suffering from sclerema, he says: “In the Moscow foundling hospital, metal cradles with double walls are used to warm up children who are not born used, in the interspaces of which warm water is continuously maintained.” However, no further information is given about these cradles.
Footnotes
[1] The measurements were taken by Dr. Â Israel, and the tables of numbers that followed later were also compiled at my instigation from the records of the institution, for which I express my heartfelt thanks to him here.
[2] “De la couveuse pour enfants” by A. Auvard, intern at The Maternité of Paris, in Archives of Tocologie, October 1883, p. 577.
[3] Centralblatt für Gynäkologie, 1882, No. 1-3.
[4] “Die Zellgewebsverhärtung der Neugeborenen,” in Oesterreichischen Jahrbuche für Pädiatrik, 1873, I, S. 30.
- Carl Siegmund Franz Credé (Wikipedia)
- Credé’s paper “Ueber Erwärmungsgeräthe für frühgeborene und schwächliche kleine Kinder” (German)
Last Updated on 03/23/23