Continuous Positive Airway Pressure (CPAP)
The story of CPAP begins with Dr. George Gregory of UCSF. Dr. Gregory made numerous contributions to neonatology and pediatric anesthesia through his research and is widely known for his textbook Gregory’s Pediatric Anesthesia, but his most important achievement is undoubtedly the invention of the use of continuous positive airway pressure (CPAP) for respiratory distress syndrome.
When Dr. Gregory was still a junior anesthesiologist on call in the NICU, he was called to see a premature infant in severe respiratory distress with a PaO2 of 30 mmHg. Without intervention, the baby would undoubtedly would have perished. Dr. Gregory recalls, “The infant was in respiratory distress and actually went to the (cardiac catheter) lab because the cardiologists thought he had congenital heart disease. He didn’t have congenital heart disease. The baby was breathing 150 times a minute, so I intubated his trachea and put an end expiratory pressure of 6–8 mmHg on the tube using a Jackson-Rees modification of the Ayres T-piece. Over the next hour, the PaO2 rose to about 230 mmHg.” [1] The child survived. Subsequently the therapy was applied to 20 infants of birthweight 930-3800 g with respiratory distress syndrome over a 16-month period, with 16 of the 20 surviving – remarkable for those days.[2]
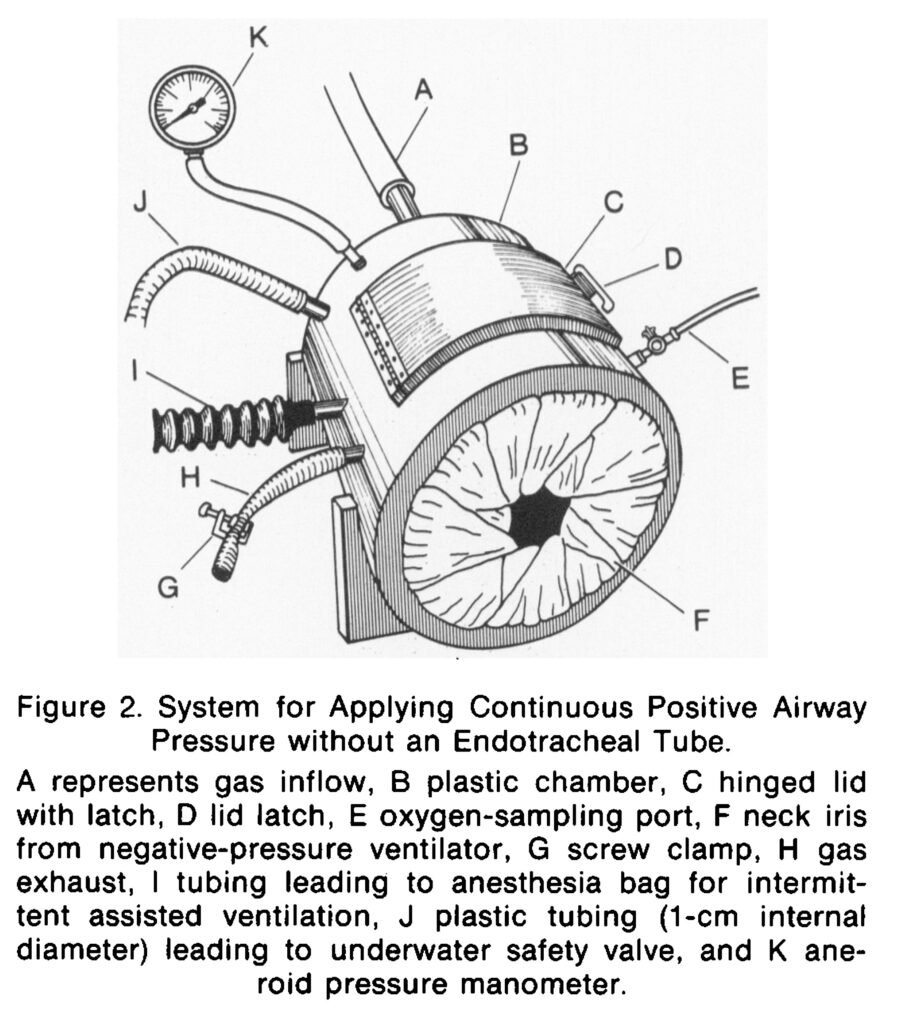
In order to avoid the trauma and risks of intubation, Dr. Gregory modified his treatment to use what was later referred to as a “Gregory Box,” or pressurized plastic chamber with the infant’s head inside, receiving an oxygen/air mixture under controlled pressure, leaving the body outside for easy access.[3] However, head boxes had their own challenges – a very loud environment for the baby, gastric distension from the babies swallowing the pressurized air, the possibility of leaks or overpressure events, and difficult access for nurses when they needed to suction the baby or do other care around the head.
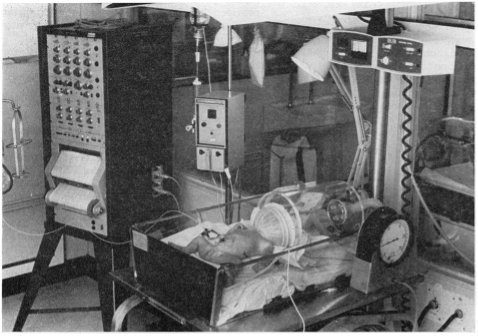
Gregory Boxes were briefly produced by Vickers Medical, in England, from around 1972 to 1974. However, many pioneering organizations with NICUs fabricated them in house.
By 1973, the teams of Dr. Kattwinkel and Dr. Agostino separately developed and published a technique for delivering CPAP using soft nasal prongs (below right) or nasal cannulas (below left) which (along with the so-called “bubble CPAP” pioneered by Sahni and Wung) remain the standard of practice today. [4] [5] [6]


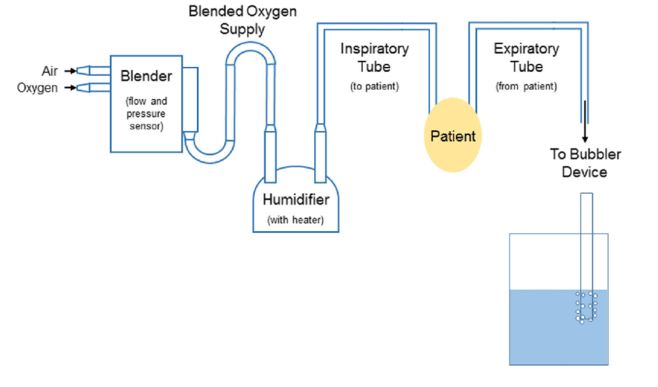
The invention of bubble CPAP significantly simplified the use of CPAP for respiratory distress syndrome. A continuous flow of air with a predetermined percentage of O2 is delivered to the infant through nasal prongs or a nasal cannula, but Instead of controlling the end-expiratory pressure with a ventilator and its associated tubing as well as its management by a respiratory therapist, the end-expiratory pressure is managed by the simple expedient of submerging the exhaust tube in a container of water. The depth of the tube in the water controls the pressure (cm of H2O) delivered. The bubbling action also creates gentle vibrations (oscillations) which may assist in gas exchange and lung recruitment.
The introduction of CPAP took place at least 5 years before the widespread availability of infant ventilators, and undoubtedly saved an untold number of lives. Such ventilators as were used at all were adult ventilators such as the MA-1 adapted with pediatric tubing, which were volume-based and poorly matched to premature infant physiology, and were usually a last resort before demise, Severe respiratory distress syndrome continued to take its toll until neonatologists could bring other technologies to bear: time-cycled pressure-limited ventilators such as the Baby Bird, and later, surfactant replacement.
[1] Mai CL, Yaster M, Firth P: “The Development of Continuous Positive Airway Pressure: an Interview with Dr. George Gregory.” Pediatric Anesthesia 23 (2013) 3-8. doi:10.1111/pan.12075
[2] Gregory GA, Kitterman JA, et al: “Treatment of the Idiopathic Respiratory Distress Syndrome with Continuous Positive Airway Pressure.” NEJM 284(24), 1333-1340. June 17, 1971.
[3] Dunn PM: “Continuous Positive Airways Pressure Using the Gregory Box.” Proceedings of the Royal Society of Medicine, (67) 245-247, May 1974.
[4] Kattwinkel J., Fleming D., Cha C. C., Fanaroff A. A., Klaus M. H. A device for administration of continuous positive airway pressure by the nasal route. Pediatrics. 1973 Jul;52(1):131–134.
[5] Caliumi-Pellegrini G., Agostino R., Orzalesi M., Nodari S., Marzetti G., Savignoni P. G., Bucci G. Twin nasal cannula for administration of continuous positive airway pressure to newborn infants. Arch Dis Child. 1974 Mar;49(3):228–230. doi: 10.1136/adc.49.3.228.
[6] 5. Sahni R, Wung J-T. Continuous positive airway pressure (CPAP). Indian J Pediatr 1998;65:265–71. 10.1007/BF02752303
Portions of this page were drafted with machine assistance; the final text was reviewed, verified, and edited by the author.
Last Updated on 07/20/26