The Budin-Pinard Obstetric Manikin
Obstetric simulation developed in the first half of the 18th century. In early 18th-century Paris, father and son surgeon-accoucheurs [obstetricians] named Grégoire offered courses in midwifery using demonstrations upon a leather-covered pelvis placed in a basketwork frame. William Smellie, a Scottish surgeon who studied under Grégoire the younger around 1738, was dissatisfied and constructed far more realistic simulators built on actual human bones covered with leather, with artificial ligaments and uteri that could contract and dilate. Around the same time, French midwife Madame du Coudray (ca. 1712–94), encouraged by Louis XV, created a wooden and canvas manikin incorporating a true bony pelvis and a newborn-sized doll, and used it to train midwives and physicians across France.
By the late 19th century, the design of obstetrical phantoms was increasingly standardized, with examples produced in large numbers by European manufacturers. Well-known models included the Budin-Pinard and its rivals: the Edgar-Parvin Obstetric Manikin designed by American obstetricians J. Clifton Edgar (1859–1939) and Theophilus Parvin (1829–98), and the Schultze Manikin created by German obstetrician B.S. Schultze (1827–1919).
The Inventors
As we have described elsewhere in individual biographical entries, Stéphane Tarnier (1828-1897) succeeded Paul Dubois as chief surgeon at La Maternité de Paris in 1867 and introduced infection control measures that reduced mortality from puerperal fever from 93 per 1000 in 1870 to 7 per 1000 in 1890. He also pioneered incubator use for preterm newborns. Both Pierre Budin (1846–1907) and Adolphe Pinard (1844–1934) were attending physicians together with Stéphane Tarnier at La Maternité in Paris, and Budin later succeeded Tarnier as professor of midwifery at the Paris Faculté de Médecine in 1898.
Budin founded the Ligue contre la mortalité infantile in 1902. In addition to his legendary accomplishments and writings as an obstetrician, he made improvements to Tarnier’s incubator and established many core concepts of premature infant care that were ahead of their time: careful tracking of weight and nutrition, use of breast milk, temperature control, gavage, and prevention of infection, among others. His book Le Nourrisson (1900) can be thought of as the first textbook of neonatology. He also pioneered the Consultations de Nourrisons, perinatal clinics promoting breastfeeding and infant hygiene.
Pinard served as accoucheur des hôpitaux at the Hôpital Lariboisière from 1882, became professor of clinical obstetrics at the Faculté de Médecine in 1890, and by 1891 was director of the Clinique Baudelocque, the newest and most technologically advanced maternity hospital in Paris. He established antenatal care as a public health necessity, created a refuge for destitute pregnant women, introduced fetal heart auscultation as a wellbeing indicator, invented the monaural fetal stethoscope, and described systematic abdominal palpation to determine fetal position.
All three were proflific, multifaceted expert physicians, authors of countless books and academic articles, teachers, and inventors. Together, Tarnier, Budin, and Pinard developed foundational elements of the obstetric care model and premature infant care used today.
Creation and First Demonstration of the Manikin
Budin and Pinard’s creation of their Obstetric Manikin or Phantom occurred at a moment of intense professional rivalry in French medicine, when the invention of new instruments was a primary means of securing professional prestige. The manikin bore a metal plate stamped “BSGDG” — Breveté Sans Garantie du Gouvernement, a type of French patent — alongside the prominently displayed inscription Mathieu, identifying its manufacturer.
Budin’s doctoral dissertation had addressed the passage of the fetal head through the pelvis (1876); Pinard’s thesis addressed congenital malformations of the pelvis (1874). Their manikin design reflects both these early research interests. Tarnier had himself designed a simpler precursor — an artificial pelvis in cast iron with a movable sacrum, manufactured by Collin & Cie (1868) — and Budin had used this model in experiments for his dissertation. The Budin-Pinard manikin built upon Tarnier’s design, retaining the adjustable sacrum but incorporating the added resistance and realism of soft rubber tissues.
The manikin’s use was also driven by a broader demographic anxiety: the 1890s in France were marked by alarm over the country’s declining birthrate and rising infant mortality, with pronatalist policies creating institutional pressure to improve the training of obstetricians and midwives.
In November 1877, at a meeting of the Obstetrical Society of London, Dr. Fancourt Barnes described and demonstrated the model developed by Budin and Pinard, using it to show application of forceps to the fetal head. The manikin had been manufactured by Mathieu fils — also known as Maison L. Mathieu or Maison Mathieu, founded in the mid-19th century by Louis-Joseph Mathieu — a well-known Paris firm of instrument makers. A month later, Tarnier exhibited the manikin on Budin and Pinard’s behalf at the French Academy of Medicine, where the first detailed drawings were published. The manikin’s professional debut was closely linked to Tarnier’s axis-traction forceps, which had been designed just that year and which made their public debut alongside the Budin-Pinard at the Exposition universelle of 1878 — underscoring the two instruments as interdependent technologies.
Design and Construction
The manikin represented the torso of a female body from just above the breasts to a few inches above the knee, placed by default in “the French obstetric position” — supine with the legs spread wide — though it could also be positioned in the English or American left lateral position. The body was hand-carved in painted wood. Soft rubber formed the abdominal walls (J), uterus (A), os uteri (U), perineum (P), and vulva (V), attached by screws. The interior was carved to replicate a normal pelvis, with a rubber lining of the abdominal and pelvic cavities molded at the outlet to form the birth canal.
A rubber bag (B) held a fresh or preserved fetal cadaver lubricated with soap or Vaseline; filled with water, it simulated a living fetus in amniotic fluid. A syringe (E) allowed users to displace air from the rubber uterus and replace it with water. A separate small cavity (C) could be filled with air to replicate the resistance of the intestines. By 1890, the design also incorporated a rubber rectum for practicing operations such as the Ritgen maneuver and perineal protection.
The key mechanical innovation was a screw mechanism on the underside of the manikin allowing the sacral promontory to be advanced to simulate varying degrees of pelvic contraction from rickets — then a common cause of obstructed labor. This enabled practice of cephalotripsy, craniotomy, and embryotomy under conditions far closer to actual anatomy than older phantoms permitted. The original screw was replaced at some later point by a “mechanism in the longitudinal axis” achieving the same effect.
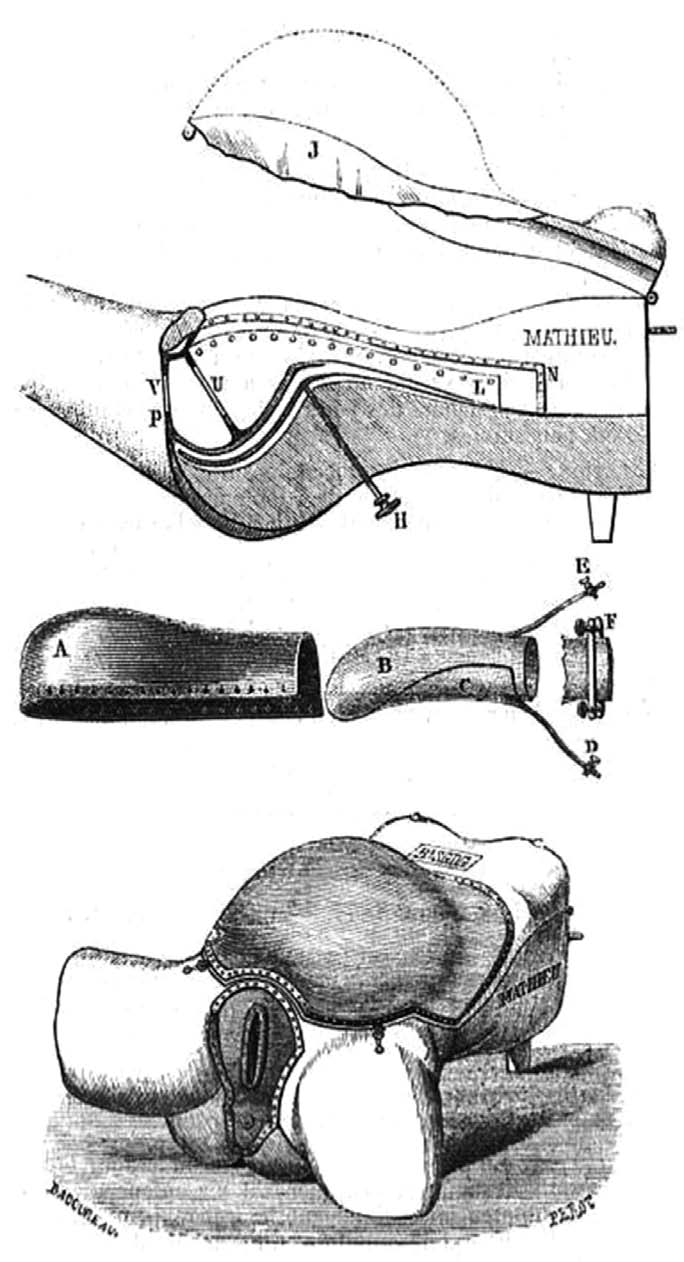
The Budin-Pinard obstetric simulator. Source: Gazette Hebdomadaire de Médecine et
de Chirurgie, December 21, 1877.
Only Budin and Pinard employed rubber for the abdominal wall, allowing students to practice external palpation — the technique Pinard had systematized in his Traité du palper abdominal (1878) — in addition to internal examinations. The rubber components were designed as consumables, replaceable when worn: an explicit design feature noted at the manikin’s very first public description.
Unlike the cadaver, the rubber manikin could be washed or sterilized between uses, preventing transmission of infection from classroom to delivery room — a significant consideration in the era of germ theory and Semmelweis. Budin even advised users to lubricate their fingers before vaginal examination on the manikin, as one would with a clinical patient.
Spread and Adoption
The manikin circulated rapidly. It appeared in Cincinnati just one year after its London debut. In 1879, Jacob Trush demonstrated it to the Obstetrical Society of Cincinnati. The College of Medicine and Surgery in Cincinnati announced in 1880–81 that it had imported the model directly from Paris. It was adopted at the University of Maryland after 1883, at McGill’s Montreal Maternity, at Georgetown University Hospital, and in Rome at l’Ospedale S. Spirito. J. Whitridge Williams of Johns Hopkins specifically recommended it in a paper on teaching obstetrics at the 1898 meeting of the Association of American Medical Colleges. Illustrations of the manikin were reproduced in French, British, Spanish, German, and American medical journals and catalogues.
By the late 19th century, the manikin was in use not only in courses for male physicians but also in women’s medical education. At the Woman’s Medical College of Pennsylvania, fourth-year students attended lectures on “Operative Obstetrics and Operative Gynæcology on the Cadaver and Manikin.” Photographic evidence from the early 20th century shows students at the college working with a Budin-Pinard manikin.
American physician Robert L. Dickinson described the full complement of equipment required for manikin instruction in 1892: “a bony pelvis, a fœtal skull, chamois fœtus, fœtal cadaver, rubber uterus, rubber amnion, rubber detachable vulva and vagina, [and] detachable abdominal walls.” He also described the use of curtained compartments in the classroom — each manikin set off by curtains — so that students could concentrate on their own station without distraction from adjacent procedures. Instructors could introduce obstetric emergencies “without warning,” inserting a fresh placenta or cord to simulate conditions such as placenta prævia or prolapsus funis. The manikin’s rubber components threatened by design to escape users’ control — fluids could burst forth, a fetus might become obstructed or slip uncontrollably through the birth canal — and this unpredictability was a deliberate pedagogical feature.
The manikin trained two distinct but related haptic skills. Budin described toucher — internal manual exploration by way of the vagina to diagnose fetal position — and palper — external abdominal palpation, potentially also therapeutic in the case of external version. Tarnier’s textbook Traité de l’art des accouchements (1882) repeatedly directed students to reproduce described positions on the manikin, pairing printed illustration with tactile training.
The obstetrical machine functioned as both a teaching tool and an instrument of professional self-fashioning. University-trained physicians secured their authority in large part through ability to perform complex maneuvers — embryotomies, forceps delivery — that midwives were legally prohibited from attempting under the French Loi du 30 novembre 1892 sur exercice de la médecine. In the United States and United Kingdom, the Comstock Act (1873) and Obscene Publications Act (1857) were used to restrict public display of anatomical models related to human reproduction, making it necessary to continually affirm the manikin’s status as a medical rather than popular object. The Budin-Pinard’s abstract, truncated design — headless, marble-white, without fashionable accessories — distinguished it deliberately from the more lurid realism of competing models such as the Edgar-Parvin full-body figure.
Commercial Availability and the Accessories Ecosystem
At Mathieu fils in Paris, the complete Budin-Pinard retailed at 500 francs; a simpler version without the movable sacrum and rubber organs cost 300 francs. An ordinary mannequin sold for 100–125 francs, placing the Budin-Pinard at a fourfold premium. In the United States, Charles H. Ward of Rochester, NY listed it in his 1902 catalogue at $200 for the full model with movable sacrum and $150 for the brevette model without it.
The Kny-Scheerer Company catalog of 1915 (pages 5053–5055, primary source) positioned the Budin-Pinard at $150 net with fetus (catalog item E/-2124) within a four-model lineup:
- E/-2120 Plain Pattern Phantom, with fœtus — $40.00
- E/-2124 Budin and Pinard’s Phantom, with fœtus — $150.00
- E/-2128 Edgar’s Phantom, complete leather-covered figure, without fœtus — $200.00
- E/-2131 Schultze’s Phantom, chamois covered, without fœtus — $75.00
The Kny-Scheerer Company, New York, “Surgical Instruments,” 20th Edition, pages 5053 and 5055.
The same catalog offered fetal simulators separately: a French Pattern Artificial Fœtus with compressible head at $20.00, Schultze’s chamois-covered model at $16.50, and a Natural Fœtal Skull at $3.50. The compressible head directly simulated cranial molding under forceps pressure. Four accessories were designated specifically for the Budin-Pinard: soft rubber vulva with perineum ($10.00), soft rubber abdomen ($10.00), inflatable soft rubber bladder and uterus ($8.50), and Deshayes’ soft rubber labia and vagina ($10.00). Equipping a full teaching station with phantom, accessories, and fetal simulator cost approximately $200–220 in 1915.
The supply of rubber parts was disrupted by World War I, affecting both cost and availability.
Longevity, Decline, and Surviving Examples
Advertisements for the Budin-Pinard appeared in medical journals and catalogues as late as 1935; it remained listed in the Kny-Scheerer catalogue through 1941 — more than 60 years after its debut. Its decline came as women increasingly delivered in hospital, where laboring patients became the primary teaching material, and as postgraduate specialization reduced the need for operative obstetrics in basic medical curricula.
The simulator is now very rare. The example at the Pelosi Medical Center in New Jersey, made by Tramond-Rouppert/Docteur Auzoux (post-1926, when Auzoux acquired Mathieu’s rival firm), has largely perished rubber parts but an intact wooden structure revealing the sacral adjustment mechanism. A second example with more intact rubber components is at the Musée Grenoblois des Sciences Médicales in Grenoble. A third has been acquired by the Musée Flaubert et d’Histoire de la Médecine in Rouen. The specimen in the Hospital Universitario de Santa Cristina (Madrid) was photographed for the institution’s 2024 centenary midwifery exhibition.

The Simulator in Modern Context
Pinard himself acknowledged in his 1891 preface to Farabeuf and Varnier’s Fundamentals of Obstetrics that the mannequin was “un simulacre imparfait” (an imperfect representation) and that practicing on cadavers was ten times superior, though expert guidance mattered regardless of teaching material. Budin noted in the atlas he co-authored with Tarnier that the manikin could not entirely duplicate the resistance of living tissues. Robert Lee, writing in 1865, warned that long practice on a phantom without attendance at difficult labors could produce a dangerous degree of boldness in practitioners who had never encountered the resistance and variability of a living patient.
The pedagogical logic of the Budin-Pinard — simulation before clinical exposure, standardized practice of rare emergencies, tactile skill development — anticipates the framework of contemporary simulation-based training. Modern successors include the Noelle (Gaumard, 2003) and SimMom (Laerdal) high-fidelity mannequins, and the BirthSIM augmented reality simulator with instrumented forceps. The Budin-Pinard’s core features — abdominal palpation training, variable pelvic geometry, replaceable components — remain relevant design considerations. Owen and Pelosi (2013) argued that the Budin-Pinard, if reconstructed in modern materials, could still serve as a valuable educational tool.
Primary sources
- “November 7th, 1877” [meeting report]. Transactions of the Obstetrical Society of London 19 (1877): 223–31.
- Tarnier M. Enseignement obstétrical [in French]. Gazette hebdomadaire de médecine et de chirurgie. 1877;14:815–816. [First detailed illustrations of the Budin-Pinard; source of Figure 1 in Owen & Pelosi.]
- DeRossett MJ, Wood TF, eds. Medical annotations: Obstetric phantoms (London Examiner, November 15). N C Med J. 1878;1(1):54–55. [First English-language description of the simulator’s design and intended use.]
- Transactions of the Obstetrical Society of Cincinnati. Amer. J. Obstet. Dis. Women Child. 13, no. 1 (January 1, 1880): 170–74. [Jacob Trush’s description of the manikin.]
- Edgar JC. The manikin in the teaching of practical obstetrics. New York Medical Journal. December 27, 1890:701–9. [Includes earliest North American illustrations of the manikin.]
- Dickinson RL. Details of a practical course of manikin instruction in obstetrics. New York Med. J. 56 (October 22, 1892): 454–58. [Description of classroom pedagogy including curtained compartments.]
- Farabeuf LH, Varnier H. Introduction à l’étude clinique et la pratique des accouchements. Paris: Georges Steinheil, 1891. [Preface by Pinard; source of “un simulacre imparfait.”]
- Ward CH. Catalogue of Human and Comparative Skeletons, Osteological Specialties, and Anatomical Models. Rochester, NY: Gillies Press, 1902. [Lists Budin-Pinard at $200/$150.]
- Kny-Scheerer Company. Illustrations of Surgical Instruments of Superior Quality, 20th ed. New York: Kny-Scheerer Corporation, 1915. [Catalog pages 5053–5055; primary source for pricing and accessories; reproduced by user.]
- Kny-Scheerer Corporation. Catalog of Surgical Instruments of Superior Quality, 25th ed. Long Island City, NY: Walters Surgical Company, 1941. [Last known US catalogue listing of the Budin-Pinard.]
- Witkowski GJ. Histoire des accouchements chez tous les peoples. Appendice: L’Arsenal obstétrical. Paris: G. Steinheil, 1887. [Source of original Budin-Pinard illustrations and Tarnier pelvis illustration.]
- Bar P. Recherches expérimentales & cliniques pour servir à l’histoire de l’embryotomie céphalique. Paris: Asselin et Houzeau, 1889. [Documents modifications to sacral mechanism and custom version by Mathieu fils.]
- Maison L. Mathieu. Liste des instruments nouveaux créés et des instruments anciens modifiés depuis l’exposition de 1878. Paris: Imprimeries réunies, 1889. [Manufacturer’s own description of the manikin; source for French franc pricing.]
- Lee R. Three Hundred Consultations in Midwifery. London; 1864. [Critical assessment of phantom training.]
Secondary sources
- Owen H, Pelosi MA. A historical examination of the Budin-Pinard phantom: what can contemporary obstetrics education learn from simulators of the past? Academic Medicine. 2013;88(5):652–6. DOI: 10.1097/ACM.0b013e31828b0464
- Dandona JM. (Re)producing Reproduction: Obstetrical Training Models and Methods, 1880–1900. Bulletin of the History of Medicine. 2025;99(1):236–273. DOI: 10.1353/bhm.2025.a963732 . Available at Project Muse: https://muse.jhu.edu/article/963732
- Owen H. Simulation in obstetrics, gynecology and midwifery. In: Comprehensive Healthcare Simulation: Obstetrics and Gynecology. Springer; 2017. [Reproduced at basicmedicalkey.com/simulation-in-obstetrics-gynecology-and-midwifery/]
- Owen H. Early use of simulation in medical education. Simulation in Healthcare. 2012;7(2):102–116.
- Lepage J, Cosson M, Mayeur O, Brieu M, Rubod C. Pedagogical childbirth simulators: utility in obstetrics. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2016;197:41–47. DOI: 10.1016/j.ejogrb.2015.11.011
- Wood W (contributor). Budin-Pinard Obstetric Manikin [item entry]. Victorian Things digital archive. University of Victoria Libraries; object dated c.1890. Available at: https://omekas.library.uvic.ca/s/crafting/item/5901
- Museo de Ecología Humana. The Budin and Pinard obstetric model [exhibit entry]. A Centenary for the Midwives of Santa Cristina. Virtual Museum of Human Ecology; 2024. Available at: https://museoecologiahumana.org/en/obras/11061-2/
Last Updated on 06/11/26